Abstract: PB1776
Type: Publication Only
Background
Hairy cell leukemia (HCL) patients have near-normal life expectancies since the introduction of purine nucleoside analogues. However, HCL remains a chronic, often relapsing disease in which maximizing treatment-free survival (TFS) is the main goal.
Aims
Prognostication is not standardized in HCL, emphasizing the relevance of the characterization of HCL populations.
Methods
We retrospectively analysed 40 patients (90% men), diagnosed between 1997 and 2016, with a median follow-up of 6 years.
Results
At presentation, the median age was 58 years and 69% of patients were symptomatic - fatigue (53%), B symptoms (50%), bleeding (14%), abdominal discomfort (6%) and severe infection (22%). The commonest cytopenia was thrombocytopenia (70%), with median platelet count being 66x10^9/L. Monocyte counts below 0.1x10^9/L were observed in 61% of the patients. Splenomegaly was observed in 83% of the patients and 21% had abdominal lymphadenopathies.
The majority of the patients (88%) was treated with cladribine in first line, achieving an overall response (OR) rate of 100% and a complete response (CR) rate of 38%, of which 67% were classified as minimal residual disease (MRD)-negative CR. Retreatment was required in 33% of the patients, of which the majority received cladribine. The median time-to-next-treatment (TNT) from first to second line was 3 years. The OR rate for second-line treatment was 91%, 50% achieving CR, of which 33% were classified as MRD-negative CR. Only 5% of the patients required further treatment lines. Even the presence of scarce hairy cells in the bone marrow precluded classification of response as CR. This might have contributed to the low CR levels observed in our patients. As post-treatment bone marrow biopsies were available in only 24 patients, response analysis was restricted to these patients. All of these 24 patients had bone marrow fibrosis at diagnosis, which reverted when and in whom first CR was obtained. Median overall survival (OS) was not reached and, at 10 years, the OS was 90%. Four deaths occurred, all unrelated to HCL.
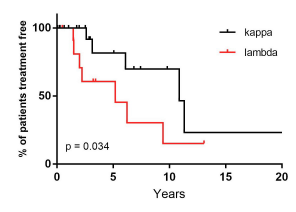
Regarding prognostication, a trend to a longer TFS, albeit no statistically significant, was observed in patients achieving CR (namely MRD negative) and without thrombocytopenia at presentation. Excitingly, the 61% of patients with kappa (k) light-chain restriction (LCR) displayed a significantly higher TFS than the 39% with lambda (λ) LCR (p 0.034, Wilcoxon-Gehan test). To the best of our knowledge, there are no published reports on prognostic value of LCR in HCL.
Conclusion
If multicentre studies corroborate our findings, LCR may be of use in the prognostication/risk stratification of HCL. Similarly with multiple myeloma and other hematological malignancies, lambda (λ) LCR appears to correlate with worse prognosis, leading to a shorter TFS.
Session topic: 6. Chronic lymphocytic leukemia and related disorders - Clinical

