
CMR FOR MYOCARDIAL IRON OVERLOAD ASSESSMENT: CALIBRATION CURVE FROM THE MIOT PROJECT
(Abstract release date: 05/19/16)
EHA Library. Meloni A. 06/09/16; 135033; PB2133

Dr. Antonella Meloni
Contributions
Contributions
Abstract
Abstract: PB2133
Type: Publication Only
Background
The measurement of myocardial iron by T2* cardiovascular magnetic resonance (CMR) has been established as fundamental to the best practice management of thalassemia. However, iron calibration data in humans is limited and CMR calibration varies according to instrumentation and technique.
Aims
The aim of this study was to calibrate the T2*-CMR technique for noninvasive cardiac iron assessment, by considering a segmental approach.
Methods
Four human hearts were studied from transfusion-dependent patients after their death within the MIOT network (Myocardial Iron Overload in Thalassemia). A multislice multiecho T2* approach was adopted. After CMR, used as guidance, the heart was cut in three short-axis slice and each slice was cut into different equiangular segments, the same ones in which the T2* was assessed. Tissue iron concentration in the segments was measured with inductively coupled plasma atomic emission spectroscopy.
Results
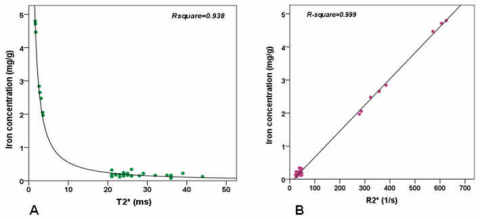
T2* and iron concentration were overall assessed in 36 myocardial segments: 6 in the first heart (year 2004), 6 in the second one (year 2004), 8 in the third one (year 2005), and 16 in the fourth one (year 2010),Figure 1A shows the segmental iron concentration (in milligrams per gram dry weight) plotted versus the correspondent segmental T2* value (in milliseconds). As expected, the relationship was not linear. In Figure 1B the R2* values (R2*=1000/T2*, in s-1) were considered. Regression analysis yielded a linear calibration of the following form: [Fe]R2* =0 .0079 × R2* - 0.1262 (R-square=0.999).
Conclusion
As in the only previously proposed calibration curve by Carpenter et al (Circulation 2011), we did not collected hearts with an intermediate iron burden. We found an excellent linear agreement between R2* and cardiac iron with a model similar to the calibration curve in the gerbil showed by Wood J et al (Circulation 2005). The results further validate the current clinical practice of monitoring cardiac iron in vivo by CMR.
Session topic: E-poster
Keyword(s): Iron overload, Magnetic resonance imaging
Type: Publication Only
Background
The measurement of myocardial iron by T2* cardiovascular magnetic resonance (CMR) has been established as fundamental to the best practice management of thalassemia. However, iron calibration data in humans is limited and CMR calibration varies according to instrumentation and technique.
Aims
The aim of this study was to calibrate the T2*-CMR technique for noninvasive cardiac iron assessment, by considering a segmental approach.
Methods
Four human hearts were studied from transfusion-dependent patients after their death within the MIOT network (Myocardial Iron Overload in Thalassemia). A multislice multiecho T2* approach was adopted. After CMR, used as guidance, the heart was cut in three short-axis slice and each slice was cut into different equiangular segments, the same ones in which the T2* was assessed. Tissue iron concentration in the segments was measured with inductively coupled plasma atomic emission spectroscopy.
Results
T2* and iron concentration were overall assessed in 36 myocardial segments: 6 in the first heart (year 2004), 6 in the second one (year 2004), 8 in the third one (year 2005), and 16 in the fourth one (year 2010),Figure 1A shows the segmental iron concentration (in milligrams per gram dry weight) plotted versus the correspondent segmental T2* value (in milliseconds). As expected, the relationship was not linear. In Figure 1B the R2* values (R2*=1000/T2*, in s-1) were considered. Regression analysis yielded a linear calibration of the following form: [Fe]R2* =0 .0079 × R2* - 0.1262 (R-square=0.999).
Conclusion
As in the only previously proposed calibration curve by Carpenter et al (Circulation 2011), we did not collected hearts with an intermediate iron burden. We found an excellent linear agreement between R2* and cardiac iron with a model similar to the calibration curve in the gerbil showed by Wood J et al (Circulation 2005). The results further validate the current clinical practice of monitoring cardiac iron in vivo by CMR.
Session topic: E-poster
Keyword(s): Iron overload, Magnetic resonance imaging
Abstract: PB2133
Type: Publication Only
Background
The measurement of myocardial iron by T2* cardiovascular magnetic resonance (CMR) has been established as fundamental to the best practice management of thalassemia. However, iron calibration data in humans is limited and CMR calibration varies according to instrumentation and technique.
Aims
The aim of this study was to calibrate the T2*-CMR technique for noninvasive cardiac iron assessment, by considering a segmental approach.
Methods
Four human hearts were studied from transfusion-dependent patients after their death within the MIOT network (Myocardial Iron Overload in Thalassemia). A multislice multiecho T2* approach was adopted. After CMR, used as guidance, the heart was cut in three short-axis slice and each slice was cut into different equiangular segments, the same ones in which the T2* was assessed. Tissue iron concentration in the segments was measured with inductively coupled plasma atomic emission spectroscopy.
Results
T2* and iron concentration were overall assessed in 36 myocardial segments: 6 in the first heart (year 2004), 6 in the second one (year 2004), 8 in the third one (year 2005), and 16 in the fourth one (year 2010),Figure 1A shows the segmental iron concentration (in milligrams per gram dry weight) plotted versus the correspondent segmental T2* value (in milliseconds). As expected, the relationship was not linear. In Figure 1B the R2* values (R2*=1000/T2*, in s-1) were considered. Regression analysis yielded a linear calibration of the following form: [Fe]R2* =0 .0079 × R2* - 0.1262 (R-square=0.999).
Conclusion
As in the only previously proposed calibration curve by Carpenter et al (Circulation 2011), we did not collected hearts with an intermediate iron burden. We found an excellent linear agreement between R2* and cardiac iron with a model similar to the calibration curve in the gerbil showed by Wood J et al (Circulation 2005). The results further validate the current clinical practice of monitoring cardiac iron in vivo by CMR.
Session topic: E-poster
Keyword(s): Iron overload, Magnetic resonance imaging
Type: Publication Only
Background
The measurement of myocardial iron by T2* cardiovascular magnetic resonance (CMR) has been established as fundamental to the best practice management of thalassemia. However, iron calibration data in humans is limited and CMR calibration varies according to instrumentation and technique.
Aims
The aim of this study was to calibrate the T2*-CMR technique for noninvasive cardiac iron assessment, by considering a segmental approach.
Methods
Four human hearts were studied from transfusion-dependent patients after their death within the MIOT network (Myocardial Iron Overload in Thalassemia). A multislice multiecho T2* approach was adopted. After CMR, used as guidance, the heart was cut in three short-axis slice and each slice was cut into different equiangular segments, the same ones in which the T2* was assessed. Tissue iron concentration in the segments was measured with inductively coupled plasma atomic emission spectroscopy.
Results
T2* and iron concentration were overall assessed in 36 myocardial segments: 6 in the first heart (year 2004), 6 in the second one (year 2004), 8 in the third one (year 2005), and 16 in the fourth one (year 2010),Figure 1A shows the segmental iron concentration (in milligrams per gram dry weight) plotted versus the correspondent segmental T2* value (in milliseconds). As expected, the relationship was not linear. In Figure 1B the R2* values (R2*=1000/T2*, in s-1) were considered. Regression analysis yielded a linear calibration of the following form: [Fe]R2* =0 .0079 × R2* - 0.1262 (R-square=0.999).
Conclusion
As in the only previously proposed calibration curve by Carpenter et al (Circulation 2011), we did not collected hearts with an intermediate iron burden. We found an excellent linear agreement between R2* and cardiac iron with a model similar to the calibration curve in the gerbil showed by Wood J et al (Circulation 2005). The results further validate the current clinical practice of monitoring cardiac iron in vivo by CMR.
Session topic: E-poster
Keyword(s): Iron overload, Magnetic resonance imaging
{{ help_message }}
{{filter}}