
ADENOTONSILLECTOMY IN SICKLE CELL DISEASE: IS TRANSFUSION NEEDED?
(Abstract release date: 05/19/16)
EHA Library. Elshinawy M. 06/09/16; 135025; PB2125

Assoc. Prof. Mohamed Elshinawy
Contributions
Contributions
Abstract
Abstract: PB2125
Type: Publication Only
Background
Adenotonsillar hypertrophy in patients with sickle cell disease (SCD) can predispose to several complications including obstructive sleep apnea, vasocclusive crisis (VOC), pulmonary hypertension, and acute chest syndrome. Traditionally, all children with sickle cell disease (SCD) indicated for adenoidectomy and/or tonsillectomy have been exposed to exchange transfusion preoperatively aiming at reduction of both surgical and SCD-related complications.
Aims
To address the need for transfusion in patients with SCD undergoing adenotonsillectomy and to report its risks and benefits.
Methods
All patients with SCD admitted in SQUH for adenotonsillectomy from July 2006 till January 2015 were included in the study. Between 2006 and 2012, patients’ files were reviewed for retrospective data recording. After 2012, the study has been prospective.
Results
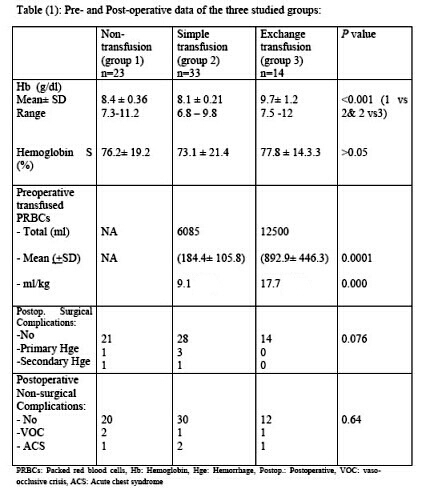
The current cohort included 70 patients with SCD. They were categorized into three groups. (No transfusion, simple transfusion and exchange transfusion group). Almost 33% of patients with SCD didn’t need any preoperative transfusion before surgery (23 out of 70 patients). There was no statistically significant difference between the 3 studied groups as regards the development of surgical or SCD related complication. Development of postoperative vaso-occlusive crisis and acute chest syndrome was comparable in the three groups. As an advantage, there was a markedly significant less blood used in patients given simple top-up transfusion as compared to exchange transfusion group. All results are shown in table 1.
Conclusion
We conclude that it is safe to do adenotonsillectomy in patients with SCD with hemoglobin above 8 g/dl without any transfusion. Exchange transfusion before surgery is not indicated and it does not improve surgical or SCD-related outcome.
Session topic: E-poster
Keyword(s): Sickle cell disease, Transfusion
Type: Publication Only
Background
Adenotonsillar hypertrophy in patients with sickle cell disease (SCD) can predispose to several complications including obstructive sleep apnea, vasocclusive crisis (VOC), pulmonary hypertension, and acute chest syndrome. Traditionally, all children with sickle cell disease (SCD) indicated for adenoidectomy and/or tonsillectomy have been exposed to exchange transfusion preoperatively aiming at reduction of both surgical and SCD-related complications.
Aims
To address the need for transfusion in patients with SCD undergoing adenotonsillectomy and to report its risks and benefits.
Methods
All patients with SCD admitted in SQUH for adenotonsillectomy from July 2006 till January 2015 were included in the study. Between 2006 and 2012, patients’ files were reviewed for retrospective data recording. After 2012, the study has been prospective.
Results
The current cohort included 70 patients with SCD. They were categorized into three groups. (No transfusion, simple transfusion and exchange transfusion group). Almost 33% of patients with SCD didn’t need any preoperative transfusion before surgery (23 out of 70 patients). There was no statistically significant difference between the 3 studied groups as regards the development of surgical or SCD related complication. Development of postoperative vaso-occlusive crisis and acute chest syndrome was comparable in the three groups. As an advantage, there was a markedly significant less blood used in patients given simple top-up transfusion as compared to exchange transfusion group. All results are shown in table 1.
Conclusion
We conclude that it is safe to do adenotonsillectomy in patients with SCD with hemoglobin above 8 g/dl without any transfusion. Exchange transfusion before surgery is not indicated and it does not improve surgical or SCD-related outcome.
Session topic: E-poster
Keyword(s): Sickle cell disease, Transfusion
Abstract: PB2125
Type: Publication Only
Background
Adenotonsillar hypertrophy in patients with sickle cell disease (SCD) can predispose to several complications including obstructive sleep apnea, vasocclusive crisis (VOC), pulmonary hypertension, and acute chest syndrome. Traditionally, all children with sickle cell disease (SCD) indicated for adenoidectomy and/or tonsillectomy have been exposed to exchange transfusion preoperatively aiming at reduction of both surgical and SCD-related complications.
Aims
To address the need for transfusion in patients with SCD undergoing adenotonsillectomy and to report its risks and benefits.
Methods
All patients with SCD admitted in SQUH for adenotonsillectomy from July 2006 till January 2015 were included in the study. Between 2006 and 2012, patients’ files were reviewed for retrospective data recording. After 2012, the study has been prospective.
Results
The current cohort included 70 patients with SCD. They were categorized into three groups. (No transfusion, simple transfusion and exchange transfusion group). Almost 33% of patients with SCD didn’t need any preoperative transfusion before surgery (23 out of 70 patients). There was no statistically significant difference between the 3 studied groups as regards the development of surgical or SCD related complication. Development of postoperative vaso-occlusive crisis and acute chest syndrome was comparable in the three groups. As an advantage, there was a markedly significant less blood used in patients given simple top-up transfusion as compared to exchange transfusion group. All results are shown in table 1.
Conclusion
We conclude that it is safe to do adenotonsillectomy in patients with SCD with hemoglobin above 8 g/dl without any transfusion. Exchange transfusion before surgery is not indicated and it does not improve surgical or SCD-related outcome.
Session topic: E-poster
Keyword(s): Sickle cell disease, Transfusion
Type: Publication Only
Background
Adenotonsillar hypertrophy in patients with sickle cell disease (SCD) can predispose to several complications including obstructive sleep apnea, vasocclusive crisis (VOC), pulmonary hypertension, and acute chest syndrome. Traditionally, all children with sickle cell disease (SCD) indicated for adenoidectomy and/or tonsillectomy have been exposed to exchange transfusion preoperatively aiming at reduction of both surgical and SCD-related complications.
Aims
To address the need for transfusion in patients with SCD undergoing adenotonsillectomy and to report its risks and benefits.
Methods
All patients with SCD admitted in SQUH for adenotonsillectomy from July 2006 till January 2015 were included in the study. Between 2006 and 2012, patients’ files were reviewed for retrospective data recording. After 2012, the study has been prospective.
Results
The current cohort included 70 patients with SCD. They were categorized into three groups. (No transfusion, simple transfusion and exchange transfusion group). Almost 33% of patients with SCD didn’t need any preoperative transfusion before surgery (23 out of 70 patients). There was no statistically significant difference between the 3 studied groups as regards the development of surgical or SCD related complication. Development of postoperative vaso-occlusive crisis and acute chest syndrome was comparable in the three groups. As an advantage, there was a markedly significant less blood used in patients given simple top-up transfusion as compared to exchange transfusion group. All results are shown in table 1.
Conclusion
We conclude that it is safe to do adenotonsillectomy in patients with SCD with hemoglobin above 8 g/dl without any transfusion. Exchange transfusion before surgery is not indicated and it does not improve surgical or SCD-related outcome.
Session topic: E-poster
Keyword(s): Sickle cell disease, Transfusion
{{ help_message }}
{{filter}}