
SHOULD STAGE I AND II FOLLICULAR LYMPHOMA BE TREATED EVEN IN THE RITUXIMAB ERA?
(Abstract release date: 05/19/16)
EHA Library. Toral Ibarra D. 06/09/16; 134770; PB1870

Dr. Dennisse Sharon Toral Ibarra
Contributions
Contributions
Abstract
Abstract: PB1870
Type: Publication Only
Background
The optimal management of stage I and II follicular lymphoma (FL), according to consensus guidelines, is not well defined, there are heterogeneous criteria to choose the option of treatment and the decision used to be based on uncontrolled experiences. Diverse treatment approaches are used because the most of guidelines recommended a broad spectrum of alternatives that includes from observation to radiotherapy or chemotherapy, without clear indications to choose one. It is still widely accepted to observe advanced stage FL in case of asymptomatic and stable disease, nevertheless, this watch-and-wait policy is not too well established in early stages. The clinical outcome of patients with follicular lymphoma has been improved since the introduction of rituximab, nevertheless the guidelines still recommend the radiotherapy as a first option.
Aims
This study was launched to evaluate the time to relapse with the three more common approaches in the Rituximab era.
Methods
All patients with histologically confirmed diagnosis of follicular lymphomas grade I-II were selected from our data base starting from January 2000 to June 2015.
Results
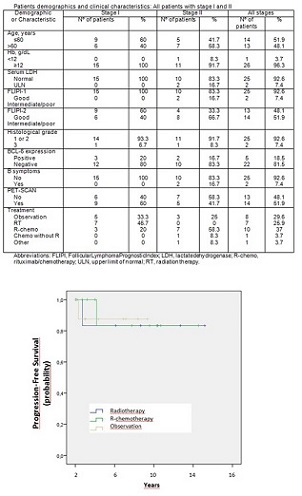
From January 2000 to June 2015, 179 patients were diagnosed of follicular lymphoma in our Institution. 35 patients were staged as I and II, 5 patients were excluded from the analysis because of not rigorous staging as defined by bone marrow biopsy and an imaging study either with computed tomography [CT] scan of the whole body or a positron emission tomography [PET]/CT scan, and 3 patients were excluded because of bulky stage II. The median age at diagnosis was 58 years (range 29-78).PET/CT was done in 52 % patients. Treatments given to staged patients were rituximab/chemotherapy (R-chemo; 37%) that includes regimes such as R-CHOP (cyclophosphamide [C], doxorubicin, vincristine [V] and prednisone [P]) R-CVP, R-FC (fludarabine [F], cyclophosphamide), chemotherapy without immunotherapy (3.7%), RT (25.9%), observation (29.6%), and other (3.7%). With a median follow-up of 70 months for PFS, there were 3 progression events (11,11% of patients). PFS was statistically significant improved with observation compared with patients treated either receiving R-QT or RT (p=0.042). There were nostatistical differences in PFS according to FLIPI 1 or 2 score, histological grade or BCL-6 expression in univariate analysis. There were not differences in overall survival.
Conclusion
This retrospective monocentric study suggest that observation could be a valid approach for patients of FL stage I and not bulky II, not only for stage III or IV. PFS did not improve with treatment, even with rituximab-containing chemotherapy regimens. It is necessary prospective and randomized studies in these cases to get stronger conclusions.
Session topic: E-poster
Keyword(s): Follicular lymphoma
Type: Publication Only
Background
The optimal management of stage I and II follicular lymphoma (FL), according to consensus guidelines, is not well defined, there are heterogeneous criteria to choose the option of treatment and the decision used to be based on uncontrolled experiences. Diverse treatment approaches are used because the most of guidelines recommended a broad spectrum of alternatives that includes from observation to radiotherapy or chemotherapy, without clear indications to choose one. It is still widely accepted to observe advanced stage FL in case of asymptomatic and stable disease, nevertheless, this watch-and-wait policy is not too well established in early stages. The clinical outcome of patients with follicular lymphoma has been improved since the introduction of rituximab, nevertheless the guidelines still recommend the radiotherapy as a first option.
Aims
This study was launched to evaluate the time to relapse with the three more common approaches in the Rituximab era.
Methods
All patients with histologically confirmed diagnosis of follicular lymphomas grade I-II were selected from our data base starting from January 2000 to June 2015.
Results
From January 2000 to June 2015, 179 patients were diagnosed of follicular lymphoma in our Institution. 35 patients were staged as I and II, 5 patients were excluded from the analysis because of not rigorous staging as defined by bone marrow biopsy and an imaging study either with computed tomography [CT] scan of the whole body or a positron emission tomography [PET]/CT scan, and 3 patients were excluded because of bulky stage II. The median age at diagnosis was 58 years (range 29-78).PET/CT was done in 52 % patients. Treatments given to staged patients were rituximab/chemotherapy (R-chemo; 37%) that includes regimes such as R-CHOP (cyclophosphamide [C], doxorubicin, vincristine [V] and prednisone [P]) R-CVP, R-FC (fludarabine [F], cyclophosphamide), chemotherapy without immunotherapy (3.7%), RT (25.9%), observation (29.6%), and other (3.7%). With a median follow-up of 70 months for PFS, there were 3 progression events (11,11% of patients). PFS was statistically significant improved with observation compared with patients treated either receiving R-QT or RT (p=0.042). There were nostatistical differences in PFS according to FLIPI 1 or 2 score, histological grade or BCL-6 expression in univariate analysis. There were not differences in overall survival.
Conclusion
This retrospective monocentric study suggest that observation could be a valid approach for patients of FL stage I and not bulky II, not only for stage III or IV. PFS did not improve with treatment, even with rituximab-containing chemotherapy regimens. It is necessary prospective and randomized studies in these cases to get stronger conclusions.
Session topic: E-poster
Keyword(s): Follicular lymphoma
Abstract: PB1870
Type: Publication Only
Background
The optimal management of stage I and II follicular lymphoma (FL), according to consensus guidelines, is not well defined, there are heterogeneous criteria to choose the option of treatment and the decision used to be based on uncontrolled experiences. Diverse treatment approaches are used because the most of guidelines recommended a broad spectrum of alternatives that includes from observation to radiotherapy or chemotherapy, without clear indications to choose one. It is still widely accepted to observe advanced stage FL in case of asymptomatic and stable disease, nevertheless, this watch-and-wait policy is not too well established in early stages. The clinical outcome of patients with follicular lymphoma has been improved since the introduction of rituximab, nevertheless the guidelines still recommend the radiotherapy as a first option.
Aims
This study was launched to evaluate the time to relapse with the three more common approaches in the Rituximab era.
Methods
All patients with histologically confirmed diagnosis of follicular lymphomas grade I-II were selected from our data base starting from January 2000 to June 2015.
Results
From January 2000 to June 2015, 179 patients were diagnosed of follicular lymphoma in our Institution. 35 patients were staged as I and II, 5 patients were excluded from the analysis because of not rigorous staging as defined by bone marrow biopsy and an imaging study either with computed tomography [CT] scan of the whole body or a positron emission tomography [PET]/CT scan, and 3 patients were excluded because of bulky stage II. The median age at diagnosis was 58 years (range 29-78).PET/CT was done in 52 % patients. Treatments given to staged patients were rituximab/chemotherapy (R-chemo; 37%) that includes regimes such as R-CHOP (cyclophosphamide [C], doxorubicin, vincristine [V] and prednisone [P]) R-CVP, R-FC (fludarabine [F], cyclophosphamide), chemotherapy without immunotherapy (3.7%), RT (25.9%), observation (29.6%), and other (3.7%). With a median follow-up of 70 months for PFS, there were 3 progression events (11,11% of patients). PFS was statistically significant improved with observation compared with patients treated either receiving R-QT or RT (p=0.042). There were nostatistical differences in PFS according to FLIPI 1 or 2 score, histological grade or BCL-6 expression in univariate analysis. There were not differences in overall survival.
Conclusion
This retrospective monocentric study suggest that observation could be a valid approach for patients of FL stage I and not bulky II, not only for stage III or IV. PFS did not improve with treatment, even with rituximab-containing chemotherapy regimens. It is necessary prospective and randomized studies in these cases to get stronger conclusions.
Session topic: E-poster
Keyword(s): Follicular lymphoma
Type: Publication Only
Background
The optimal management of stage I and II follicular lymphoma (FL), according to consensus guidelines, is not well defined, there are heterogeneous criteria to choose the option of treatment and the decision used to be based on uncontrolled experiences. Diverse treatment approaches are used because the most of guidelines recommended a broad spectrum of alternatives that includes from observation to radiotherapy or chemotherapy, without clear indications to choose one. It is still widely accepted to observe advanced stage FL in case of asymptomatic and stable disease, nevertheless, this watch-and-wait policy is not too well established in early stages. The clinical outcome of patients with follicular lymphoma has been improved since the introduction of rituximab, nevertheless the guidelines still recommend the radiotherapy as a first option.
Aims
This study was launched to evaluate the time to relapse with the three more common approaches in the Rituximab era.
Methods
All patients with histologically confirmed diagnosis of follicular lymphomas grade I-II were selected from our data base starting from January 2000 to June 2015.
Results
From January 2000 to June 2015, 179 patients were diagnosed of follicular lymphoma in our Institution. 35 patients were staged as I and II, 5 patients were excluded from the analysis because of not rigorous staging as defined by bone marrow biopsy and an imaging study either with computed tomography [CT] scan of the whole body or a positron emission tomography [PET]/CT scan, and 3 patients were excluded because of bulky stage II. The median age at diagnosis was 58 years (range 29-78).PET/CT was done in 52 % patients. Treatments given to staged patients were rituximab/chemotherapy (R-chemo; 37%) that includes regimes such as R-CHOP (cyclophosphamide [C], doxorubicin, vincristine [V] and prednisone [P]) R-CVP, R-FC (fludarabine [F], cyclophosphamide), chemotherapy without immunotherapy (3.7%), RT (25.9%), observation (29.6%), and other (3.7%). With a median follow-up of 70 months for PFS, there were 3 progression events (11,11% of patients). PFS was statistically significant improved with observation compared with patients treated either receiving R-QT or RT (p=0.042). There were nostatistical differences in PFS according to FLIPI 1 or 2 score, histological grade or BCL-6 expression in univariate analysis. There were not differences in overall survival.
Conclusion
This retrospective monocentric study suggest that observation could be a valid approach for patients of FL stage I and not bulky II, not only for stage III or IV. PFS did not improve with treatment, even with rituximab-containing chemotherapy regimens. It is necessary prospective and randomized studies in these cases to get stronger conclusions.
Session topic: E-poster
Keyword(s): Follicular lymphoma
{{ help_message }}
{{filter}}