
DONOR-TRANSMITTED TRIPLE-HIT LYMPHOMA IN A RENAL ALLOGRAFT RECIPIENT
(Abstract release date: 05/19/16)
EHA Library. Biavati L. 06/09/16; 134623; PB1723

Mr. Luca Biavati
Contributions
Contributions
Abstract
Abstract: PB1723
Type: Publication Only
Background
Donor cancer transmission is a rare long-term complication of kidney transplantation that carries an estimated risk of approximately 0.05%. Diagnosis and management of these malignancies are difficult because of their rarity and the need for an individualized approach to treatment. CM is a 30-years-old man with a medical history significant for chronic kidney disease who underwent kidney transplantation in May 2015 with his mother as the donor. In July 2015, the donor presented with an abdominal mass diagnosed as a triple-hit lymphoma (THL), a subset of highly aggressive B-cell lymphomas characterized by the overexpression of MYC, BCL2 and BCL6. Initial staging with PET/CT and bone marrow biopsy showed widespread disease with no marrow involvement, while circulating tumor DNA (ctDNA) assay confirmed a clonal B-cell proliferation. Analysis of ctDNA was performed on recipient’s plasma, but ctDNA levels were undetectable. In September 2015, CM developed a perigraft mass that was identified as a THL as well. The peculiar clinical presentation and the histochemical similarities of the two THLs raised the suspicion that the same lymphoma had been transmitted from the donor to the recipient during the transplant procedure.
Aims
This case describes donor transmission of THL with kidney transplantation and points out difficulties in diagnosis and management.
Methods
Lymphoma biopsy specimens from both donor and recipient were obtained and prepared for histological and immunohistochemical (IHC) studies and stained for the identification of Ki67, CD20, BCL6, BCL2, MYC, CD10, MUM1/IRF4, CD5, cyclin D1, CD3, EBV-LMP1 and TdT. DNA was extracted from the biopsies of both donor and recipient THL with standard methods. Samples were assessed for nine microsatellite loci and a segment of the X-Y homologous gene amelogenin by PCR with use of a kit for chimerism determination. Fluorescent in-situ hybridization (FISH) studies were performed on specimen sections using probes for sex determination. B-cell clonality analyses targeting the IGH gene for rearrangements were conducted on ctDNA obtained from plasma of both donor and recipient and from the recipient’s bone marrow.
Results
Histology and IHC showed identical findings in both donor and recipient. In particular, MYC, BCL2 and BCL6 were positive and the proliferative index was more than 90%. FISH recognized an XX pattern in both samples. Microchimerism analysis pointed out that the donor and the recipient biopsies had identical profiles considering discriminant alleles and amelogenin (see Figure). Moreover, the recipient sample profile was significantly different from his basal allelic profile obtained from peripheral lymphocytes at the time of the diagnosis. B-cell clonality in the donor sample was detected at the time of the diagnosis, however ctDNA levels assessed on recipient’s sample were undetectable. The same clonal band was persistently detected by ctDNA analysis of the recipient plasma and bone marrow only after September 2015.
Conclusion
We describe the transmission of a highly aggressive B-cell non-Hodgkin lymphoma by kidney transplantation. The THL was transplanted along with the renal graft, while immunosuppressive therapy and immunological impairment enabled its growth and expansion. The patient went on to complete the full course of 2 cycles of R CODOXM/IVAC and associated withdrawal of immunosuppression achieving a complete remission and preserving graft function. The donor underwent the same intensive regimen and achieved a complete response as well.
Session topic: E-poster
Keyword(s): BCL2, Chimerism, MYC, Transplant
Type: Publication Only
Background
Donor cancer transmission is a rare long-term complication of kidney transplantation that carries an estimated risk of approximately 0.05%. Diagnosis and management of these malignancies are difficult because of their rarity and the need for an individualized approach to treatment. CM is a 30-years-old man with a medical history significant for chronic kidney disease who underwent kidney transplantation in May 2015 with his mother as the donor. In July 2015, the donor presented with an abdominal mass diagnosed as a triple-hit lymphoma (THL), a subset of highly aggressive B-cell lymphomas characterized by the overexpression of MYC, BCL2 and BCL6. Initial staging with PET/CT and bone marrow biopsy showed widespread disease with no marrow involvement, while circulating tumor DNA (ctDNA) assay confirmed a clonal B-cell proliferation. Analysis of ctDNA was performed on recipient’s plasma, but ctDNA levels were undetectable. In September 2015, CM developed a perigraft mass that was identified as a THL as well. The peculiar clinical presentation and the histochemical similarities of the two THLs raised the suspicion that the same lymphoma had been transmitted from the donor to the recipient during the transplant procedure.
Aims
This case describes donor transmission of THL with kidney transplantation and points out difficulties in diagnosis and management.
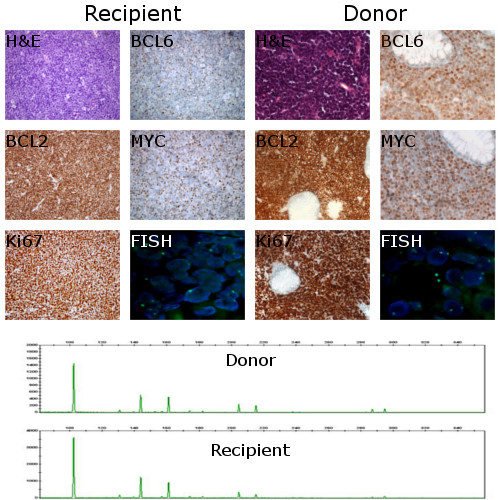
Methods
Lymphoma biopsy specimens from both donor and recipient were obtained and prepared for histological and immunohistochemical (IHC) studies and stained for the identification of Ki67, CD20, BCL6, BCL2, MYC, CD10, MUM1/IRF4, CD5, cyclin D1, CD3, EBV-LMP1 and TdT. DNA was extracted from the biopsies of both donor and recipient THL with standard methods. Samples were assessed for nine microsatellite loci and a segment of the X-Y homologous gene amelogenin by PCR with use of a kit for chimerism determination. Fluorescent in-situ hybridization (FISH) studies were performed on specimen sections using probes for sex determination. B-cell clonality analyses targeting the IGH gene for rearrangements were conducted on ctDNA obtained from plasma of both donor and recipient and from the recipient’s bone marrow.
Results
Histology and IHC showed identical findings in both donor and recipient. In particular, MYC, BCL2 and BCL6 were positive and the proliferative index was more than 90%. FISH recognized an XX pattern in both samples. Microchimerism analysis pointed out that the donor and the recipient biopsies had identical profiles considering discriminant alleles and amelogenin (see Figure). Moreover, the recipient sample profile was significantly different from his basal allelic profile obtained from peripheral lymphocytes at the time of the diagnosis. B-cell clonality in the donor sample was detected at the time of the diagnosis, however ctDNA levels assessed on recipient’s sample were undetectable. The same clonal band was persistently detected by ctDNA analysis of the recipient plasma and bone marrow only after September 2015.
Conclusion
We describe the transmission of a highly aggressive B-cell non-Hodgkin lymphoma by kidney transplantation. The THL was transplanted along with the renal graft, while immunosuppressive therapy and immunological impairment enabled its growth and expansion. The patient went on to complete the full course of 2 cycles of R CODOXM/IVAC and associated withdrawal of immunosuppression achieving a complete remission and preserving graft function. The donor underwent the same intensive regimen and achieved a complete response as well.
Session topic: E-poster
Keyword(s): BCL2, Chimerism, MYC, Transplant
Abstract: PB1723
Type: Publication Only
Background
Donor cancer transmission is a rare long-term complication of kidney transplantation that carries an estimated risk of approximately 0.05%. Diagnosis and management of these malignancies are difficult because of their rarity and the need for an individualized approach to treatment. CM is a 30-years-old man with a medical history significant for chronic kidney disease who underwent kidney transplantation in May 2015 with his mother as the donor. In July 2015, the donor presented with an abdominal mass diagnosed as a triple-hit lymphoma (THL), a subset of highly aggressive B-cell lymphomas characterized by the overexpression of MYC, BCL2 and BCL6. Initial staging with PET/CT and bone marrow biopsy showed widespread disease with no marrow involvement, while circulating tumor DNA (ctDNA) assay confirmed a clonal B-cell proliferation. Analysis of ctDNA was performed on recipient’s plasma, but ctDNA levels were undetectable. In September 2015, CM developed a perigraft mass that was identified as a THL as well. The peculiar clinical presentation and the histochemical similarities of the two THLs raised the suspicion that the same lymphoma had been transmitted from the donor to the recipient during the transplant procedure.
Aims
This case describes donor transmission of THL with kidney transplantation and points out difficulties in diagnosis and management.
Methods
Lymphoma biopsy specimens from both donor and recipient were obtained and prepared for histological and immunohistochemical (IHC) studies and stained for the identification of Ki67, CD20, BCL6, BCL2, MYC, CD10, MUM1/IRF4, CD5, cyclin D1, CD3, EBV-LMP1 and TdT. DNA was extracted from the biopsies of both donor and recipient THL with standard methods. Samples were assessed for nine microsatellite loci and a segment of the X-Y homologous gene amelogenin by PCR with use of a kit for chimerism determination. Fluorescent in-situ hybridization (FISH) studies were performed on specimen sections using probes for sex determination. B-cell clonality analyses targeting the IGH gene for rearrangements were conducted on ctDNA obtained from plasma of both donor and recipient and from the recipient’s bone marrow.
Results
Histology and IHC showed identical findings in both donor and recipient. In particular, MYC, BCL2 and BCL6 were positive and the proliferative index was more than 90%. FISH recognized an XX pattern in both samples. Microchimerism analysis pointed out that the donor and the recipient biopsies had identical profiles considering discriminant alleles and amelogenin (see Figure). Moreover, the recipient sample profile was significantly different from his basal allelic profile obtained from peripheral lymphocytes at the time of the diagnosis. B-cell clonality in the donor sample was detected at the time of the diagnosis, however ctDNA levels assessed on recipient’s sample were undetectable. The same clonal band was persistently detected by ctDNA analysis of the recipient plasma and bone marrow only after September 2015.
Conclusion
We describe the transmission of a highly aggressive B-cell non-Hodgkin lymphoma by kidney transplantation. The THL was transplanted along with the renal graft, while immunosuppressive therapy and immunological impairment enabled its growth and expansion. The patient went on to complete the full course of 2 cycles of R CODOXM/IVAC and associated withdrawal of immunosuppression achieving a complete remission and preserving graft function. The donor underwent the same intensive regimen and achieved a complete response as well.
Session topic: E-poster
Keyword(s): BCL2, Chimerism, MYC, Transplant
Type: Publication Only
Background
Donor cancer transmission is a rare long-term complication of kidney transplantation that carries an estimated risk of approximately 0.05%. Diagnosis and management of these malignancies are difficult because of their rarity and the need for an individualized approach to treatment. CM is a 30-years-old man with a medical history significant for chronic kidney disease who underwent kidney transplantation in May 2015 with his mother as the donor. In July 2015, the donor presented with an abdominal mass diagnosed as a triple-hit lymphoma (THL), a subset of highly aggressive B-cell lymphomas characterized by the overexpression of MYC, BCL2 and BCL6. Initial staging with PET/CT and bone marrow biopsy showed widespread disease with no marrow involvement, while circulating tumor DNA (ctDNA) assay confirmed a clonal B-cell proliferation. Analysis of ctDNA was performed on recipient’s plasma, but ctDNA levels were undetectable. In September 2015, CM developed a perigraft mass that was identified as a THL as well. The peculiar clinical presentation and the histochemical similarities of the two THLs raised the suspicion that the same lymphoma had been transmitted from the donor to the recipient during the transplant procedure.
Aims
This case describes donor transmission of THL with kidney transplantation and points out difficulties in diagnosis and management.
Methods
Lymphoma biopsy specimens from both donor and recipient were obtained and prepared for histological and immunohistochemical (IHC) studies and stained for the identification of Ki67, CD20, BCL6, BCL2, MYC, CD10, MUM1/IRF4, CD5, cyclin D1, CD3, EBV-LMP1 and TdT. DNA was extracted from the biopsies of both donor and recipient THL with standard methods. Samples were assessed for nine microsatellite loci and a segment of the X-Y homologous gene amelogenin by PCR with use of a kit for chimerism determination. Fluorescent in-situ hybridization (FISH) studies were performed on specimen sections using probes for sex determination. B-cell clonality analyses targeting the IGH gene for rearrangements were conducted on ctDNA obtained from plasma of both donor and recipient and from the recipient’s bone marrow.
Results
Histology and IHC showed identical findings in both donor and recipient. In particular, MYC, BCL2 and BCL6 were positive and the proliferative index was more than 90%. FISH recognized an XX pattern in both samples. Microchimerism analysis pointed out that the donor and the recipient biopsies had identical profiles considering discriminant alleles and amelogenin (see Figure). Moreover, the recipient sample profile was significantly different from his basal allelic profile obtained from peripheral lymphocytes at the time of the diagnosis. B-cell clonality in the donor sample was detected at the time of the diagnosis, however ctDNA levels assessed on recipient’s sample were undetectable. The same clonal band was persistently detected by ctDNA analysis of the recipient plasma and bone marrow only after September 2015.
Conclusion
We describe the transmission of a highly aggressive B-cell non-Hodgkin lymphoma by kidney transplantation. The THL was transplanted along with the renal graft, while immunosuppressive therapy and immunological impairment enabled its growth and expansion. The patient went on to complete the full course of 2 cycles of R CODOXM/IVAC and associated withdrawal of immunosuppression achieving a complete remission and preserving graft function. The donor underwent the same intensive regimen and achieved a complete response as well.
Session topic: E-poster
Keyword(s): BCL2, Chimerism, MYC, Transplant
{{ help_message }}
{{filter}}