
EFFICACY OF GEMCITABINE AS SALVAGE THERAPY FOR RELAPSED/REFRACTORY AGGRESSIVE NON HODGKIN LYMPHOMA PATIENTS
(Abstract release date: 05/19/16)
EHA Library. Kedmi M. 06/09/16; 134610; PB1710

Dr. Meirav Kedmi
Contributions
Contributions
Abstract
Abstract: PB1710
Type: Publication Only
Background
High-dose therapy with stem-cell support (ASCT) is the standard treatment for relapsed non-hodgkin lymphoma (NHL), but is not feasible for elderly or frail patients. Gemcitabine-based salvage regimens were previously shown to be an effective treatment option with response rates as high as 80% accompanied by a relatively benign toxicity profile. Our local policy is to use these regimens either for frail patients that are not eligible for ASCT, or for relapse post ASCT.
Aims
Since we had the clinical impression that our success rates are lower than the reported, we decided to retrospectively analyze the outcome of NHL patients that were treated with gemcitabine-based regimens in our institute.
Methods
Based on local pharmacy query we annotated 35 patients that were treated with gemcitabine-based regimens between 1/2007-1/2015 for relapsed/refractory aggressive NHL. Clinical features and outcomes were evaluated using thorough medical record review. Statistical analysis was done using Chi square test and Kaplan-Meier method.
Results
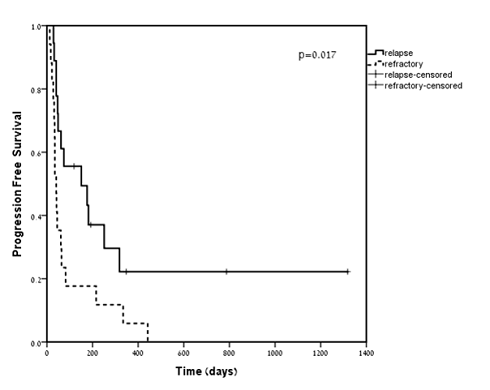
The study cohort included 23 males and 12 females. Median age was 67.2 (28-83). Median follow-up from gemcitabine initiation was 8.7 months (0.4-48.7). The most frequently used protocol was gemcitabine-oxaliplatinum (77%, n=27). Eighty percent of patients (n=28) received full dose while 20% (n=7) received reduced dose regimens. Twenty-seven patients had B cell and 8 had T cell lymphoma. All patients received a median of 2 prior regimens (1-5), of which at least 1 was anthracycline-based therapy. Seventeen patients (49%) had relapsed while 18 (51%) had refractory disease. Overall response rate (ORR) was 37%, with 29% (n=10) CR, 8% (n=3) PR, and 63% (n= 22) PD or SD. Of the 13 responders, 8 patients (61%) experienced relapse or progression during follow up. Median PFS was 61 days (range 12-1318), median OS was 23.7 months (0.4-48.7). Sixteen patients (45%) deceased during follow up. Grade 3-4 hematological-toxicity was reported in 17 patients (49%). Hospitalization due to treatment induced toxicity occurred in 12 patients (34%). Eight due to infections, 2 due to bleeding, 1 due to trauma and 1 due to abdominal pain.Several factors were tested as predictors of PFS: number of previous treatement regimens, dose intensity (full vs reduced), cell of origin, length of prior remission and relapsed vs refractory disease. The only predictor for better PFS was relapsed vs refractory disease (median 151 vs 41 days p=0.017).
Conclusion
compared to previous published data in relapsed/refractory aggressive NHL, we observed less favorable outcome along with worse toxicity. Although ORR was 37%, the median PFS after gemcitabine-based regimens was dismal (61 days). The only predictor for better PFS was relapsed as oposed to refractoy disease. Notabely, the 4 long term survivors were all treated in first (n=3) or second relapse (n=1) and received full dose regimen.Our single institution results are inferior than the published literature . The admnistration of gemcitabine based therapy as salvage regimen for patients with relasped /refractory NHL was with limited success. Innovative therapies are urgently in need for this devastating patient population as well as randomized studies.
Session topic: E-poster
Keyword(s): Gemcitabine, Non-Hodgkin's lymphoma, Toxicity
Type: Publication Only
Background
High-dose therapy with stem-cell support (ASCT) is the standard treatment for relapsed non-hodgkin lymphoma (NHL), but is not feasible for elderly or frail patients. Gemcitabine-based salvage regimens were previously shown to be an effective treatment option with response rates as high as 80% accompanied by a relatively benign toxicity profile. Our local policy is to use these regimens either for frail patients that are not eligible for ASCT, or for relapse post ASCT.
Aims
Since we had the clinical impression that our success rates are lower than the reported, we decided to retrospectively analyze the outcome of NHL patients that were treated with gemcitabine-based regimens in our institute.
Methods
Based on local pharmacy query we annotated 35 patients that were treated with gemcitabine-based regimens between 1/2007-1/2015 for relapsed/refractory aggressive NHL. Clinical features and outcomes were evaluated using thorough medical record review. Statistical analysis was done using Chi square test and Kaplan-Meier method.
Results
The study cohort included 23 males and 12 females. Median age was 67.2 (28-83). Median follow-up from gemcitabine initiation was 8.7 months (0.4-48.7). The most frequently used protocol was gemcitabine-oxaliplatinum (77%, n=27). Eighty percent of patients (n=28) received full dose while 20% (n=7) received reduced dose regimens. Twenty-seven patients had B cell and 8 had T cell lymphoma. All patients received a median of 2 prior regimens (1-5), of which at least 1 was anthracycline-based therapy. Seventeen patients (49%) had relapsed while 18 (51%) had refractory disease. Overall response rate (ORR) was 37%, with 29% (n=10) CR, 8% (n=3) PR, and 63% (n= 22) PD or SD. Of the 13 responders, 8 patients (61%) experienced relapse or progression during follow up. Median PFS was 61 days (range 12-1318), median OS was 23.7 months (0.4-48.7). Sixteen patients (45%) deceased during follow up. Grade 3-4 hematological-toxicity was reported in 17 patients (49%). Hospitalization due to treatment induced toxicity occurred in 12 patients (34%). Eight due to infections, 2 due to bleeding, 1 due to trauma and 1 due to abdominal pain.Several factors were tested as predictors of PFS: number of previous treatement regimens, dose intensity (full vs reduced), cell of origin, length of prior remission and relapsed vs refractory disease. The only predictor for better PFS was relapsed vs refractory disease (median 151 vs 41 days p=0.017).
Conclusion
compared to previous published data in relapsed/refractory aggressive NHL, we observed less favorable outcome along with worse toxicity. Although ORR was 37%, the median PFS after gemcitabine-based regimens was dismal (61 days). The only predictor for better PFS was relapsed as oposed to refractoy disease. Notabely, the 4 long term survivors were all treated in first (n=3) or second relapse (n=1) and received full dose regimen.Our single institution results are inferior than the published literature . The admnistration of gemcitabine based therapy as salvage regimen for patients with relasped /refractory NHL was with limited success. Innovative therapies are urgently in need for this devastating patient population as well as randomized studies.
Session topic: E-poster
Keyword(s): Gemcitabine, Non-Hodgkin's lymphoma, Toxicity
Abstract: PB1710
Type: Publication Only
Background
High-dose therapy with stem-cell support (ASCT) is the standard treatment for relapsed non-hodgkin lymphoma (NHL), but is not feasible for elderly or frail patients. Gemcitabine-based salvage regimens were previously shown to be an effective treatment option with response rates as high as 80% accompanied by a relatively benign toxicity profile. Our local policy is to use these regimens either for frail patients that are not eligible for ASCT, or for relapse post ASCT.
Aims
Since we had the clinical impression that our success rates are lower than the reported, we decided to retrospectively analyze the outcome of NHL patients that were treated with gemcitabine-based regimens in our institute.
Methods
Based on local pharmacy query we annotated 35 patients that were treated with gemcitabine-based regimens between 1/2007-1/2015 for relapsed/refractory aggressive NHL. Clinical features and outcomes were evaluated using thorough medical record review. Statistical analysis was done using Chi square test and Kaplan-Meier method.
Results
The study cohort included 23 males and 12 females. Median age was 67.2 (28-83). Median follow-up from gemcitabine initiation was 8.7 months (0.4-48.7). The most frequently used protocol was gemcitabine-oxaliplatinum (77%, n=27). Eighty percent of patients (n=28) received full dose while 20% (n=7) received reduced dose regimens. Twenty-seven patients had B cell and 8 had T cell lymphoma. All patients received a median of 2 prior regimens (1-5), of which at least 1 was anthracycline-based therapy. Seventeen patients (49%) had relapsed while 18 (51%) had refractory disease. Overall response rate (ORR) was 37%, with 29% (n=10) CR, 8% (n=3) PR, and 63% (n= 22) PD or SD. Of the 13 responders, 8 patients (61%) experienced relapse or progression during follow up. Median PFS was 61 days (range 12-1318), median OS was 23.7 months (0.4-48.7). Sixteen patients (45%) deceased during follow up. Grade 3-4 hematological-toxicity was reported in 17 patients (49%). Hospitalization due to treatment induced toxicity occurred in 12 patients (34%). Eight due to infections, 2 due to bleeding, 1 due to trauma and 1 due to abdominal pain.Several factors were tested as predictors of PFS: number of previous treatement regimens, dose intensity (full vs reduced), cell of origin, length of prior remission and relapsed vs refractory disease. The only predictor for better PFS was relapsed vs refractory disease (median 151 vs 41 days p=0.017).
Conclusion
compared to previous published data in relapsed/refractory aggressive NHL, we observed less favorable outcome along with worse toxicity. Although ORR was 37%, the median PFS after gemcitabine-based regimens was dismal (61 days). The only predictor for better PFS was relapsed as oposed to refractoy disease. Notabely, the 4 long term survivors were all treated in first (n=3) or second relapse (n=1) and received full dose regimen.Our single institution results are inferior than the published literature . The admnistration of gemcitabine based therapy as salvage regimen for patients with relasped /refractory NHL was with limited success. Innovative therapies are urgently in need for this devastating patient population as well as randomized studies.
Session topic: E-poster
Keyword(s): Gemcitabine, Non-Hodgkin's lymphoma, Toxicity
Type: Publication Only
Background
High-dose therapy with stem-cell support (ASCT) is the standard treatment for relapsed non-hodgkin lymphoma (NHL), but is not feasible for elderly or frail patients. Gemcitabine-based salvage regimens were previously shown to be an effective treatment option with response rates as high as 80% accompanied by a relatively benign toxicity profile. Our local policy is to use these regimens either for frail patients that are not eligible for ASCT, or for relapse post ASCT.
Aims
Since we had the clinical impression that our success rates are lower than the reported, we decided to retrospectively analyze the outcome of NHL patients that were treated with gemcitabine-based regimens in our institute.
Methods
Based on local pharmacy query we annotated 35 patients that were treated with gemcitabine-based regimens between 1/2007-1/2015 for relapsed/refractory aggressive NHL. Clinical features and outcomes were evaluated using thorough medical record review. Statistical analysis was done using Chi square test and Kaplan-Meier method.
Results
The study cohort included 23 males and 12 females. Median age was 67.2 (28-83). Median follow-up from gemcitabine initiation was 8.7 months (0.4-48.7). The most frequently used protocol was gemcitabine-oxaliplatinum (77%, n=27). Eighty percent of patients (n=28) received full dose while 20% (n=7) received reduced dose regimens. Twenty-seven patients had B cell and 8 had T cell lymphoma. All patients received a median of 2 prior regimens (1-5), of which at least 1 was anthracycline-based therapy. Seventeen patients (49%) had relapsed while 18 (51%) had refractory disease. Overall response rate (ORR) was 37%, with 29% (n=10) CR, 8% (n=3) PR, and 63% (n= 22) PD or SD. Of the 13 responders, 8 patients (61%) experienced relapse or progression during follow up. Median PFS was 61 days (range 12-1318), median OS was 23.7 months (0.4-48.7). Sixteen patients (45%) deceased during follow up. Grade 3-4 hematological-toxicity was reported in 17 patients (49%). Hospitalization due to treatment induced toxicity occurred in 12 patients (34%). Eight due to infections, 2 due to bleeding, 1 due to trauma and 1 due to abdominal pain.Several factors were tested as predictors of PFS: number of previous treatement regimens, dose intensity (full vs reduced), cell of origin, length of prior remission and relapsed vs refractory disease. The only predictor for better PFS was relapsed vs refractory disease (median 151 vs 41 days p=0.017).
Conclusion
compared to previous published data in relapsed/refractory aggressive NHL, we observed less favorable outcome along with worse toxicity. Although ORR was 37%, the median PFS after gemcitabine-based regimens was dismal (61 days). The only predictor for better PFS was relapsed as oposed to refractoy disease. Notabely, the 4 long term survivors were all treated in first (n=3) or second relapse (n=1) and received full dose regimen.Our single institution results are inferior than the published literature . The admnistration of gemcitabine based therapy as salvage regimen for patients with relasped /refractory NHL was with limited success. Innovative therapies are urgently in need for this devastating patient population as well as randomized studies.
Session topic: E-poster
Keyword(s): Gemcitabine, Non-Hodgkin's lymphoma, Toxicity
{{ help_message }}
{{filter}}