
A COMPARISON STUDY BETWEEN ALLOGENEIC AND AUTOLOGOUS HEMATOPOIETIC STEM CELL TRANSPLANT FOR HIGH-RISK PERIPHERAL T-CELL LYMPHOMAS (PTCL)
(Abstract release date: 05/19/16)
EHA Library. Huang H. 06/09/16; 134581; PB1681

Dr. Haiwen Huang
Contributions
Contributions
Abstract
Abstract: PB1681
Type: Publication Only
Background
Peripheral T-cell lymphomas (PTCLs) are heterogeneous malignancies sharing common elements of chemotherapy resistance and poor outcome with standard treatments. Attempts to improve outcomes have included autologous or allogeneic hematopoietic cell transplantation (autoHCT or alloHCT). both modalities lead to durable remissions in recurrent disease settings and might be important in consolidating first remission. However, key questions remain, including relative efficacy of autologous versus allogeneic approaches, and HCT timing (first-line consolidation v relapse).
Aims
Herein, we analyzed outcomes of 60 cases recieved autoHCT or alloHCT in our center.
Methods
From July 2007 to July 2014, Outcomes of 60 patients undergoing autologous HCT (autoHCT) or allogeneic HCT (alloHCT) were analyzed retrospectively. Primary outcomes were nonrelapse mortality (NRM), relapse/progression, progression-free survival (PFS), and overall survival (OS).
Results
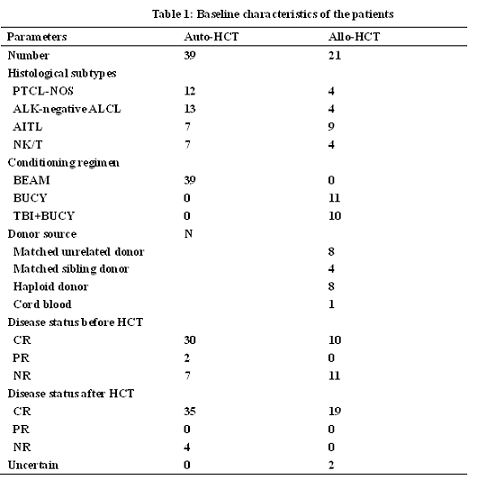
All 60 patients were at high risk group (carried with IPI≥3), with a median age of 31 (13-55) years old. Of the 60 cases, 22 were PTCL-not otherwise specified (PTCL-NOS), 22 with ALK negative anaplastic large cell lymphoma (ALK-negative ALCL) and 16 with angioimmunoblastic T-cell lymphoma (AITL). Before receiving transplantation, 40/60 patients were in complete remission (CR) and 20/60 patients were not remission (NR). Twenty-one (21/60) received allo-HSCT and thirty-nine patients (39/60) received auto-HSCT. In the 20 NR patients before transplant, 11 patients received allo-HCT and 9 patients received auto-HCT. After a median follow-up of 39 (range 1-96) months, the K-M analysis showed that the 5-year PFS for auto-HSCT and allo-HSCT were 61% and 60% (P = 0.724). 1-year NRM was higher (22.5% v 7.8%) for alloHCT. The 5-year OS for auto-HCT and allo-HCT were 62% and 61% (P = 0.724). There were no statistically significant differences between the auto-HSCT and allo-HSCT. However, autoHCT recipients were more likely in complete remission (CR; 76.9% v 47.6%; P <0.01) and with chemotherapy-sensitive disease.
Conclusion
Both autoHCT and alloHCT approaches can benefit patients with PTCL. We did not find a difference in PFS and OS between autoHCT and alloHCT, although NRM increased significantly in alloHCT. However, our results suggest that outcomes of alloHCT are better for refractory and relapsed patients with PTCL. nd overall survival (OS).
Session topic: E-poster
Keyword(s): Allogeneic hematopoietic stem cell transplant, Autologous hematopoietic stem cell transplantation, High risk, Peripheral T-cell lymphoma
Type: Publication Only
Background
Peripheral T-cell lymphomas (PTCLs) are heterogeneous malignancies sharing common elements of chemotherapy resistance and poor outcome with standard treatments. Attempts to improve outcomes have included autologous or allogeneic hematopoietic cell transplantation (autoHCT or alloHCT). both modalities lead to durable remissions in recurrent disease settings and might be important in consolidating first remission. However, key questions remain, including relative efficacy of autologous versus allogeneic approaches, and HCT timing (first-line consolidation v relapse).
Aims
Herein, we analyzed outcomes of 60 cases recieved autoHCT or alloHCT in our center.
Methods
From July 2007 to July 2014, Outcomes of 60 patients undergoing autologous HCT (autoHCT) or allogeneic HCT (alloHCT) were analyzed retrospectively. Primary outcomes were nonrelapse mortality (NRM), relapse/progression, progression-free survival (PFS), and overall survival (OS).
Results
All 60 patients were at high risk group (carried with IPI≥3), with a median age of 31 (13-55) years old. Of the 60 cases, 22 were PTCL-not otherwise specified (PTCL-NOS), 22 with ALK negative anaplastic large cell lymphoma (ALK-negative ALCL) and 16 with angioimmunoblastic T-cell lymphoma (AITL). Before receiving transplantation, 40/60 patients were in complete remission (CR) and 20/60 patients were not remission (NR). Twenty-one (21/60) received allo-HSCT and thirty-nine patients (39/60) received auto-HSCT. In the 20 NR patients before transplant, 11 patients received allo-HCT and 9 patients received auto-HCT. After a median follow-up of 39 (range 1-96) months, the K-M analysis showed that the 5-year PFS for auto-HSCT and allo-HSCT were 61% and 60% (P = 0.724). 1-year NRM was higher (22.5% v 7.8%) for alloHCT. The 5-year OS for auto-HCT and allo-HCT were 62% and 61% (P = 0.724). There were no statistically significant differences between the auto-HSCT and allo-HSCT. However, autoHCT recipients were more likely in complete remission (CR; 76.9% v 47.6%; P <0.01) and with chemotherapy-sensitive disease.
Conclusion
Both autoHCT and alloHCT approaches can benefit patients with PTCL. We did not find a difference in PFS and OS between autoHCT and alloHCT, although NRM increased significantly in alloHCT. However, our results suggest that outcomes of alloHCT are better for refractory and relapsed patients with PTCL. nd overall survival (OS).
Session topic: E-poster
Keyword(s): Allogeneic hematopoietic stem cell transplant, Autologous hematopoietic stem cell transplantation, High risk, Peripheral T-cell lymphoma
Abstract: PB1681
Type: Publication Only
Background
Peripheral T-cell lymphomas (PTCLs) are heterogeneous malignancies sharing common elements of chemotherapy resistance and poor outcome with standard treatments. Attempts to improve outcomes have included autologous or allogeneic hematopoietic cell transplantation (autoHCT or alloHCT). both modalities lead to durable remissions in recurrent disease settings and might be important in consolidating first remission. However, key questions remain, including relative efficacy of autologous versus allogeneic approaches, and HCT timing (first-line consolidation v relapse).
Aims
Herein, we analyzed outcomes of 60 cases recieved autoHCT or alloHCT in our center.
Methods
From July 2007 to July 2014, Outcomes of 60 patients undergoing autologous HCT (autoHCT) or allogeneic HCT (alloHCT) were analyzed retrospectively. Primary outcomes were nonrelapse mortality (NRM), relapse/progression, progression-free survival (PFS), and overall survival (OS).
Results
All 60 patients were at high risk group (carried with IPI≥3), with a median age of 31 (13-55) years old. Of the 60 cases, 22 were PTCL-not otherwise specified (PTCL-NOS), 22 with ALK negative anaplastic large cell lymphoma (ALK-negative ALCL) and 16 with angioimmunoblastic T-cell lymphoma (AITL). Before receiving transplantation, 40/60 patients were in complete remission (CR) and 20/60 patients were not remission (NR). Twenty-one (21/60) received allo-HSCT and thirty-nine patients (39/60) received auto-HSCT. In the 20 NR patients before transplant, 11 patients received allo-HCT and 9 patients received auto-HCT. After a median follow-up of 39 (range 1-96) months, the K-M analysis showed that the 5-year PFS for auto-HSCT and allo-HSCT were 61% and 60% (P = 0.724). 1-year NRM was higher (22.5% v 7.8%) for alloHCT. The 5-year OS for auto-HCT and allo-HCT were 62% and 61% (P = 0.724). There were no statistically significant differences between the auto-HSCT and allo-HSCT. However, autoHCT recipients were more likely in complete remission (CR; 76.9% v 47.6%; P <0.01) and with chemotherapy-sensitive disease.
Conclusion
Both autoHCT and alloHCT approaches can benefit patients with PTCL. We did not find a difference in PFS and OS between autoHCT and alloHCT, although NRM increased significantly in alloHCT. However, our results suggest that outcomes of alloHCT are better for refractory and relapsed patients with PTCL. nd overall survival (OS).
Session topic: E-poster
Keyword(s): Allogeneic hematopoietic stem cell transplant, Autologous hematopoietic stem cell transplantation, High risk, Peripheral T-cell lymphoma
Type: Publication Only
Background
Peripheral T-cell lymphomas (PTCLs) are heterogeneous malignancies sharing common elements of chemotherapy resistance and poor outcome with standard treatments. Attempts to improve outcomes have included autologous or allogeneic hematopoietic cell transplantation (autoHCT or alloHCT). both modalities lead to durable remissions in recurrent disease settings and might be important in consolidating first remission. However, key questions remain, including relative efficacy of autologous versus allogeneic approaches, and HCT timing (first-line consolidation v relapse).
Aims
Herein, we analyzed outcomes of 60 cases recieved autoHCT or alloHCT in our center.
Methods
From July 2007 to July 2014, Outcomes of 60 patients undergoing autologous HCT (autoHCT) or allogeneic HCT (alloHCT) were analyzed retrospectively. Primary outcomes were nonrelapse mortality (NRM), relapse/progression, progression-free survival (PFS), and overall survival (OS).
Results
All 60 patients were at high risk group (carried with IPI≥3), with a median age of 31 (13-55) years old. Of the 60 cases, 22 were PTCL-not otherwise specified (PTCL-NOS), 22 with ALK negative anaplastic large cell lymphoma (ALK-negative ALCL) and 16 with angioimmunoblastic T-cell lymphoma (AITL). Before receiving transplantation, 40/60 patients were in complete remission (CR) and 20/60 patients were not remission (NR). Twenty-one (21/60) received allo-HSCT and thirty-nine patients (39/60) received auto-HSCT. In the 20 NR patients before transplant, 11 patients received allo-HCT and 9 patients received auto-HCT. After a median follow-up of 39 (range 1-96) months, the K-M analysis showed that the 5-year PFS for auto-HSCT and allo-HSCT were 61% and 60% (P = 0.724). 1-year NRM was higher (22.5% v 7.8%) for alloHCT. The 5-year OS for auto-HCT and allo-HCT were 62% and 61% (P = 0.724). There were no statistically significant differences between the auto-HSCT and allo-HSCT. However, autoHCT recipients were more likely in complete remission (CR; 76.9% v 47.6%; P <0.01) and with chemotherapy-sensitive disease.
Conclusion
Both autoHCT and alloHCT approaches can benefit patients with PTCL. We did not find a difference in PFS and OS between autoHCT and alloHCT, although NRM increased significantly in alloHCT. However, our results suggest that outcomes of alloHCT are better for refractory and relapsed patients with PTCL. nd overall survival (OS).
Session topic: E-poster
Keyword(s): Allogeneic hematopoietic stem cell transplant, Autologous hematopoietic stem cell transplantation, High risk, Peripheral T-cell lymphoma
{{ help_message }}
{{filter}}