
ACUTE LYMPHOBLASTIC LEUKEMIA: A REPORT OF TWO CASES WITH THE RARE E1A3 BCR/ABL FUSION PROTEIN
(Abstract release date: 05/19/16)
EHA Library. Sartori F. 06/09/16; 134497; PB1597

Dr. Francesca Sartori
Contributions
Contributions
Abstract
Abstract: PB1597
Type: Publication Only
Background
The Philadelphia chromosome is the result of a reciprocal translocation between chromosome 22 and chromosome 9 that juxtaposes the breakpoint cluster region (BCR) to the Abelson tyrosine kinase protein. Several variants exist depending of the breakpoint in the BCR gene, being the more known ones p210, p230 and p190 bcr-abl which is the most frequently associated with ALL. Other rare variants exists (e1a3, b2a3, e6a2) the e1a3 is created by the fusion of BCR exon 1 to ABL exon 3. The molecular prognostic of these rare variant forms is still unclear.
Aims
We report two cases of adult B-ALL Ph+ bearing the rare BCR/ABL fusion protein e1a3. It is important that our lab is able to detect these variants of unclear prognosis.
Methods
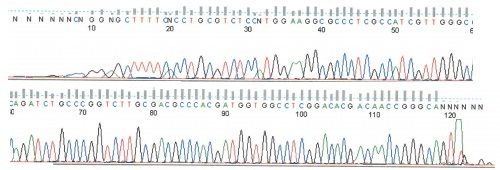
The first patient is a 43 years old man who presented this blood test: leukocytes 136,00 x 10 3/uL, Hemoglobin 11,70gr/dL, platelets 39,70 x 10 3/uL. In the peripheral blood smear 93% of small-medium sized lymphoblasts. The bone marrow aspirate confirmed the infiltration of 90% lymphoblasts; the immunophenotype was: CD19+ CD10+ CD34+ TdT+ DR+ CD79 alfa+ CD20- Cytoplasm IgM negative CD33+. The cytogenetic analysis of the BMA revealed the karyotype: 46,XY,del(9)(p22)t(9;22)(q34;q11),del(20)(q13) which confirm the diagnosis of B-ALL Ph+.Patient underwent induction chemotherapy plus imatinib reaching a morphological CR with persistence of Ph+. Currently is candidate to an allogenic SCT as consolidation. The second patient is a 65 year old man whose blood test revealed: leukocytes 223,00 10 3/uL, hemoglobin 11,60 gr/dL and platelets 118 10 3/uL. In the peripheral blood smear: 80% lymphoblasts confirmed by the immunophenotype CD19+ CD34+ DR+ CD10+ CD22+ low intensity CD20- TdT+ Cytoplasmatic IgM negative CD33+. The BMA confirmed an infiltration of 25% lymphoblasts. The cytogenetic analysis showed the karyotype: 46,XY,t(9;22)(q34;q11). He started induction therapy plus imatib; because of refractory disease is currently ongoing reinduction. He’s not candidate to SCT because of his un-fit status.In both cases the molecular analysis detected the presence of the BCR-ABL e1a3 variant. Our lab procedure isolates patient RNA from peripheral blood and is subjected to a two round multiplex RT-PCR reaction. In order to avoid RNA quality and/or handling errors, we included an internal positive control in which a 690-bp segment of the ubiquitously expressed transcription factor E2A mRNA was amplified. The primers and PCR conditions used in the first and second round of the nested PCR reaction are described by Pallisgaard et al. We identified an atypical amplification band of approximately 100 bp. In order to confirm the presence of a BCR-ABL transcript this band was extracted from the agarose gel, purified and then analyzed by DNA sequencing. cDNA sequence confirmed the presence of the e1a3 BCR-ABL transcripts.
Results
Reviewing the literature we found 20 cases bearing the e1a3 fusion proteins already described: 14 patients with B-ALL, 5 with CML and 1 patient first diagnosed with CML who experienced a B-ALL type blast crisis. Among the B-ALL patients, 8 are reported dead. It should be studied if this variant correlates to a worse prognosis, which is currently unknown.
Conclusion
We add to the literature two new cases of patients with B-ALL bearing the rare BCR/ABL fusion protein underlining the importance of detecting it; this variant could be missed in the laboratory testing giving a false negative; its role is unclear but seems to have a worse prognosis. More studies have to be done in order to understand the prognosis of this rare variant.
Session topic: E-poster
Keyword(s): Acute lymphoblastic leukemia, BCR-ABL
Type: Publication Only
Background
The Philadelphia chromosome is the result of a reciprocal translocation between chromosome 22 and chromosome 9 that juxtaposes the breakpoint cluster region (BCR) to the Abelson tyrosine kinase protein. Several variants exist depending of the breakpoint in the BCR gene, being the more known ones p210, p230 and p190 bcr-abl which is the most frequently associated with ALL. Other rare variants exists (e1a3, b2a3, e6a2) the e1a3 is created by the fusion of BCR exon 1 to ABL exon 3. The molecular prognostic of these rare variant forms is still unclear.
Aims
We report two cases of adult B-ALL Ph+ bearing the rare BCR/ABL fusion protein e1a3. It is important that our lab is able to detect these variants of unclear prognosis.
Methods
The first patient is a 43 years old man who presented this blood test: leukocytes 136,00 x 10 3/uL, Hemoglobin 11,70gr/dL, platelets 39,70 x 10 3/uL. In the peripheral blood smear 93% of small-medium sized lymphoblasts. The bone marrow aspirate confirmed the infiltration of 90% lymphoblasts; the immunophenotype was: CD19+ CD10+ CD34+ TdT+ DR+ CD79 alfa+ CD20- Cytoplasm IgM negative CD33+. The cytogenetic analysis of the BMA revealed the karyotype: 46,XY,del(9)(p22)t(9;22)(q34;q11),del(20)(q13) which confirm the diagnosis of B-ALL Ph+.Patient underwent induction chemotherapy plus imatinib reaching a morphological CR with persistence of Ph+. Currently is candidate to an allogenic SCT as consolidation. The second patient is a 65 year old man whose blood test revealed: leukocytes 223,00 10 3/uL, hemoglobin 11,60 gr/dL and platelets 118 10 3/uL. In the peripheral blood smear: 80% lymphoblasts confirmed by the immunophenotype CD19+ CD34+ DR+ CD10+ CD22+ low intensity CD20- TdT+ Cytoplasmatic IgM negative CD33+. The BMA confirmed an infiltration of 25% lymphoblasts. The cytogenetic analysis showed the karyotype: 46,XY,t(9;22)(q34;q11). He started induction therapy plus imatib; because of refractory disease is currently ongoing reinduction. He’s not candidate to SCT because of his un-fit status.In both cases the molecular analysis detected the presence of the BCR-ABL e1a3 variant. Our lab procedure isolates patient RNA from peripheral blood and is subjected to a two round multiplex RT-PCR reaction. In order to avoid RNA quality and/or handling errors, we included an internal positive control in which a 690-bp segment of the ubiquitously expressed transcription factor E2A mRNA was amplified. The primers and PCR conditions used in the first and second round of the nested PCR reaction are described by Pallisgaard et al. We identified an atypical amplification band of approximately 100 bp. In order to confirm the presence of a BCR-ABL transcript this band was extracted from the agarose gel, purified and then analyzed by DNA sequencing. cDNA sequence confirmed the presence of the e1a3 BCR-ABL transcripts.
Results
Reviewing the literature we found 20 cases bearing the e1a3 fusion proteins already described: 14 patients with B-ALL, 5 with CML and 1 patient first diagnosed with CML who experienced a B-ALL type blast crisis. Among the B-ALL patients, 8 are reported dead. It should be studied if this variant correlates to a worse prognosis, which is currently unknown.
Conclusion
We add to the literature two new cases of patients with B-ALL bearing the rare BCR/ABL fusion protein underlining the importance of detecting it; this variant could be missed in the laboratory testing giving a false negative; its role is unclear but seems to have a worse prognosis. More studies have to be done in order to understand the prognosis of this rare variant.
Session topic: E-poster
Keyword(s): Acute lymphoblastic leukemia, BCR-ABL
Abstract: PB1597
Type: Publication Only
Background
The Philadelphia chromosome is the result of a reciprocal translocation between chromosome 22 and chromosome 9 that juxtaposes the breakpoint cluster region (BCR) to the Abelson tyrosine kinase protein. Several variants exist depending of the breakpoint in the BCR gene, being the more known ones p210, p230 and p190 bcr-abl which is the most frequently associated with ALL. Other rare variants exists (e1a3, b2a3, e6a2) the e1a3 is created by the fusion of BCR exon 1 to ABL exon 3. The molecular prognostic of these rare variant forms is still unclear.
Aims
We report two cases of adult B-ALL Ph+ bearing the rare BCR/ABL fusion protein e1a3. It is important that our lab is able to detect these variants of unclear prognosis.
Methods
The first patient is a 43 years old man who presented this blood test: leukocytes 136,00 x 10 3/uL, Hemoglobin 11,70gr/dL, platelets 39,70 x 10 3/uL. In the peripheral blood smear 93% of small-medium sized lymphoblasts. The bone marrow aspirate confirmed the infiltration of 90% lymphoblasts; the immunophenotype was: CD19+ CD10+ CD34+ TdT+ DR+ CD79 alfa+ CD20- Cytoplasm IgM negative CD33+. The cytogenetic analysis of the BMA revealed the karyotype: 46,XY,del(9)(p22)t(9;22)(q34;q11),del(20)(q13) which confirm the diagnosis of B-ALL Ph+.Patient underwent induction chemotherapy plus imatinib reaching a morphological CR with persistence of Ph+. Currently is candidate to an allogenic SCT as consolidation. The second patient is a 65 year old man whose blood test revealed: leukocytes 223,00 10 3/uL, hemoglobin 11,60 gr/dL and platelets 118 10 3/uL. In the peripheral blood smear: 80% lymphoblasts confirmed by the immunophenotype CD19+ CD34+ DR+ CD10+ CD22+ low intensity CD20- TdT+ Cytoplasmatic IgM negative CD33+. The BMA confirmed an infiltration of 25% lymphoblasts. The cytogenetic analysis showed the karyotype: 46,XY,t(9;22)(q34;q11). He started induction therapy plus imatib; because of refractory disease is currently ongoing reinduction. He’s not candidate to SCT because of his un-fit status.In both cases the molecular analysis detected the presence of the BCR-ABL e1a3 variant. Our lab procedure isolates patient RNA from peripheral blood and is subjected to a two round multiplex RT-PCR reaction. In order to avoid RNA quality and/or handling errors, we included an internal positive control in which a 690-bp segment of the ubiquitously expressed transcription factor E2A mRNA was amplified. The primers and PCR conditions used in the first and second round of the nested PCR reaction are described by Pallisgaard et al. We identified an atypical amplification band of approximately 100 bp. In order to confirm the presence of a BCR-ABL transcript this band was extracted from the agarose gel, purified and then analyzed by DNA sequencing. cDNA sequence confirmed the presence of the e1a3 BCR-ABL transcripts.
Results
Reviewing the literature we found 20 cases bearing the e1a3 fusion proteins already described: 14 patients with B-ALL, 5 with CML and 1 patient first diagnosed with CML who experienced a B-ALL type blast crisis. Among the B-ALL patients, 8 are reported dead. It should be studied if this variant correlates to a worse prognosis, which is currently unknown.
Conclusion
We add to the literature two new cases of patients with B-ALL bearing the rare BCR/ABL fusion protein underlining the importance of detecting it; this variant could be missed in the laboratory testing giving a false negative; its role is unclear but seems to have a worse prognosis. More studies have to be done in order to understand the prognosis of this rare variant.
Session topic: E-poster
Keyword(s): Acute lymphoblastic leukemia, BCR-ABL
Type: Publication Only
Background
The Philadelphia chromosome is the result of a reciprocal translocation between chromosome 22 and chromosome 9 that juxtaposes the breakpoint cluster region (BCR) to the Abelson tyrosine kinase protein. Several variants exist depending of the breakpoint in the BCR gene, being the more known ones p210, p230 and p190 bcr-abl which is the most frequently associated with ALL. Other rare variants exists (e1a3, b2a3, e6a2) the e1a3 is created by the fusion of BCR exon 1 to ABL exon 3. The molecular prognostic of these rare variant forms is still unclear.
Aims
We report two cases of adult B-ALL Ph+ bearing the rare BCR/ABL fusion protein e1a3. It is important that our lab is able to detect these variants of unclear prognosis.
Methods
The first patient is a 43 years old man who presented this blood test: leukocytes 136,00 x 10 3/uL, Hemoglobin 11,70gr/dL, platelets 39,70 x 10 3/uL. In the peripheral blood smear 93% of small-medium sized lymphoblasts. The bone marrow aspirate confirmed the infiltration of 90% lymphoblasts; the immunophenotype was: CD19+ CD10+ CD34+ TdT+ DR+ CD79 alfa+ CD20- Cytoplasm IgM negative CD33+. The cytogenetic analysis of the BMA revealed the karyotype: 46,XY,del(9)(p22)t(9;22)(q34;q11),del(20)(q13) which confirm the diagnosis of B-ALL Ph+.Patient underwent induction chemotherapy plus imatinib reaching a morphological CR with persistence of Ph+. Currently is candidate to an allogenic SCT as consolidation. The second patient is a 65 year old man whose blood test revealed: leukocytes 223,00 10 3/uL, hemoglobin 11,60 gr/dL and platelets 118 10 3/uL. In the peripheral blood smear: 80% lymphoblasts confirmed by the immunophenotype CD19+ CD34+ DR+ CD10+ CD22+ low intensity CD20- TdT+ Cytoplasmatic IgM negative CD33+. The BMA confirmed an infiltration of 25% lymphoblasts. The cytogenetic analysis showed the karyotype: 46,XY,t(9;22)(q34;q11). He started induction therapy plus imatib; because of refractory disease is currently ongoing reinduction. He’s not candidate to SCT because of his un-fit status.In both cases the molecular analysis detected the presence of the BCR-ABL e1a3 variant. Our lab procedure isolates patient RNA from peripheral blood and is subjected to a two round multiplex RT-PCR reaction. In order to avoid RNA quality and/or handling errors, we included an internal positive control in which a 690-bp segment of the ubiquitously expressed transcription factor E2A mRNA was amplified. The primers and PCR conditions used in the first and second round of the nested PCR reaction are described by Pallisgaard et al. We identified an atypical amplification band of approximately 100 bp. In order to confirm the presence of a BCR-ABL transcript this band was extracted from the agarose gel, purified and then analyzed by DNA sequencing. cDNA sequence confirmed the presence of the e1a3 BCR-ABL transcripts.
Results
Reviewing the literature we found 20 cases bearing the e1a3 fusion proteins already described: 14 patients with B-ALL, 5 with CML and 1 patient first diagnosed with CML who experienced a B-ALL type blast crisis. Among the B-ALL patients, 8 are reported dead. It should be studied if this variant correlates to a worse prognosis, which is currently unknown.
Conclusion
We add to the literature two new cases of patients with B-ALL bearing the rare BCR/ABL fusion protein underlining the importance of detecting it; this variant could be missed in the laboratory testing giving a false negative; its role is unclear but seems to have a worse prognosis. More studies have to be done in order to understand the prognosis of this rare variant.
Session topic: E-poster
Keyword(s): Acute lymphoblastic leukemia, BCR-ABL
{{ help_message }}
{{filter}}