
COULD GRAFT VERSUS TUMOR EFFECT IMPROVE OUTCOMES IN MYELOID MALIGNANCIES WITH ACTIVE DISEASE UNDERGOING REDUCE INTENSITY ALLOGENEIC TRANSPLANT?
(Abstract release date: 05/19/16)
EHA Library. López-Godino O. 06/09/16; 133058; E1509

Mrs. Oriana López-Godino
Contributions
Contributions
Abstract
Abstract: E1509
Type: Eposter Presentation
Background
Allo-transplant (allo-HSCT) has become a significant treatment for refractory and relapsed haematological malignances; however, relapse remains a mayor cause of treatment failure. Reduce intensity conditioning (RIC) regimens have shown to be safe and effective in older patients or with comorbidities, but patients with chemorefractory disease still have high relapse rates and poor outcomes. Although graft versus tumor effect (GVT) has been demonstrated in some malignancies, the benefit for relapsed acute myeloid leukaemia (AML) and myelodisplastic syndrome (MDS) is often limited because of its rapid growth.
Aims
Analysis of patients with myeloid malignancies (including AML, MDS and secondary myelofibrosis) receiving RIC allo-HSCT with or without complete response (CR) in terms of transplant related mortality (TRM), event free survival (EFS) and overall survival (OS) in order to investigate the GVT in both groups.
Methods
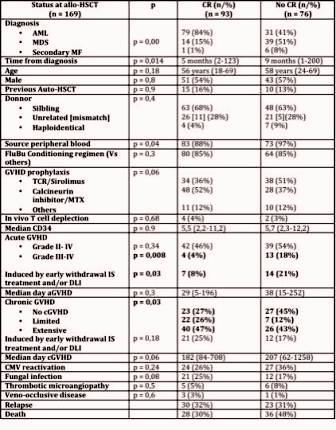
We analysed 169 patients who underwent to allo-HSCT in our centre between 1995-2015. Characteristics of both groups are described on table 1. Although cytogenetic abnormalities are not available at this moment, the data is been recording and this variable will be included in the final analysis.
Results
In the overall series and with a median follow-up of 36 months for patients alive, the estimated OS and EFS at one year, two years and five years was 71%, 64% and 58% and 61%, 51% and 45% respectively. The mainly cause of death was relapse in 32 patients (19%) and 25 (15%) due to TRM. In the Kaplan-Meier analysis the variables associated with OS (p<0,05) were: CR status, III-IV acute graft versus host disease (GVHD), development of cGVHD, fungal infection, thrombotic microangiopathy and veno-occlussive disease while just the development of cGVHD (p=0,001) with differences between grades: limited (p=0,046, HR 0,37, 0,14-0,98) and extensive (p=0,00, HR 0,24, 0,11- 0,52) and development of thrombotic microangiopathy (p=0,004, HR 4,6, 1,6-12,8), but not CR status at the moment of allo-HSCT (p=0,49), maintained significance in multivariate analysis.Regarding the outcomes on the basis of disease status at transplant, there were differences between CR and not CR patients in terms of OS (p=0,02, not achieved vs 32 months) and EFS (p=0,012; 71 Vs 9 months) but there where no differences in PFS (p=0,6); attending the TRM (p=0,05, estimated 8% Vs 22% at 1 year), there were differences manly due to the GVHD related mortality (p=0,05; 2% Vs 17% at 1 year). Exploring the GVT in both groups separately: in the group of patients with CR, there were differences between patients without cGVHD compared with patients with limited or extensive cGVHD (p=0,00) with median OS not achieved in all groups; but in those patients without CR, just extensive cGVHD seems to be effective (p = 0,00) with a median OS not achieved Vs 10 and 28 months in those patients without and with limited cGVHD respectively.
Conclusion
In our series, the PFS of patients without CR at the moment of transplant was similar to those with CR, but the first group had worse OS, EFS and higher TRM due to a larger rate of severe acute GVHD with a high proportion of induced GVHD because the early withdrawal of the immunosuppressive treatment. On the other hand, patients without CR and development of extensive cGVHD had long term survival rates, similar to those patients with CR, reflecting the GVT. Efforts should be focus on avoid severe aGVHD maintaining the GVT in order to improve the TRM rates with new immunosuppressive strategies and improve the management of minimal residual disease.
Session topic: E-poster
Keyword(s): Acute myeloid leukemia, Graft-versus-tumor effect, Myelodysplasia, Reduced intensity transplantation
Type: Eposter Presentation
Background
Allo-transplant (allo-HSCT) has become a significant treatment for refractory and relapsed haematological malignances; however, relapse remains a mayor cause of treatment failure. Reduce intensity conditioning (RIC) regimens have shown to be safe and effective in older patients or with comorbidities, but patients with chemorefractory disease still have high relapse rates and poor outcomes. Although graft versus tumor effect (GVT) has been demonstrated in some malignancies, the benefit for relapsed acute myeloid leukaemia (AML) and myelodisplastic syndrome (MDS) is often limited because of its rapid growth.
Aims
Analysis of patients with myeloid malignancies (including AML, MDS and secondary myelofibrosis) receiving RIC allo-HSCT with or without complete response (CR) in terms of transplant related mortality (TRM), event free survival (EFS) and overall survival (OS) in order to investigate the GVT in both groups.
Methods
We analysed 169 patients who underwent to allo-HSCT in our centre between 1995-2015. Characteristics of both groups are described on table 1. Although cytogenetic abnormalities are not available at this moment, the data is been recording and this variable will be included in the final analysis.
Results
In the overall series and with a median follow-up of 36 months for patients alive, the estimated OS and EFS at one year, two years and five years was 71%, 64% and 58% and 61%, 51% and 45% respectively. The mainly cause of death was relapse in 32 patients (19%) and 25 (15%) due to TRM. In the Kaplan-Meier analysis the variables associated with OS (p<0,05) were: CR status, III-IV acute graft versus host disease (GVHD), development of cGVHD, fungal infection, thrombotic microangiopathy and veno-occlussive disease while just the development of cGVHD (p=0,001) with differences between grades: limited (p=0,046, HR 0,37, 0,14-0,98) and extensive (p=0,00, HR 0,24, 0,11- 0,52) and development of thrombotic microangiopathy (p=0,004, HR 4,6, 1,6-12,8), but not CR status at the moment of allo-HSCT (p=0,49), maintained significance in multivariate analysis.Regarding the outcomes on the basis of disease status at transplant, there were differences between CR and not CR patients in terms of OS (p=0,02, not achieved vs 32 months) and EFS (p=0,012; 71 Vs 9 months) but there where no differences in PFS (p=0,6); attending the TRM (p=0,05, estimated 8% Vs 22% at 1 year), there were differences manly due to the GVHD related mortality (p=0,05; 2% Vs 17% at 1 year). Exploring the GVT in both groups separately: in the group of patients with CR, there were differences between patients without cGVHD compared with patients with limited or extensive cGVHD (p=0,00) with median OS not achieved in all groups; but in those patients without CR, just extensive cGVHD seems to be effective (p = 0,00) with a median OS not achieved Vs 10 and 28 months in those patients without and with limited cGVHD respectively.
Conclusion
In our series, the PFS of patients without CR at the moment of transplant was similar to those with CR, but the first group had worse OS, EFS and higher TRM due to a larger rate of severe acute GVHD with a high proportion of induced GVHD because the early withdrawal of the immunosuppressive treatment. On the other hand, patients without CR and development of extensive cGVHD had long term survival rates, similar to those patients with CR, reflecting the GVT. Efforts should be focus on avoid severe aGVHD maintaining the GVT in order to improve the TRM rates with new immunosuppressive strategies and improve the management of minimal residual disease.
Session topic: E-poster
Keyword(s): Acute myeloid leukemia, Graft-versus-tumor effect, Myelodysplasia, Reduced intensity transplantation
Abstract: E1509
Type: Eposter Presentation
Background
Allo-transplant (allo-HSCT) has become a significant treatment for refractory and relapsed haematological malignances; however, relapse remains a mayor cause of treatment failure. Reduce intensity conditioning (RIC) regimens have shown to be safe and effective in older patients or with comorbidities, but patients with chemorefractory disease still have high relapse rates and poor outcomes. Although graft versus tumor effect (GVT) has been demonstrated in some malignancies, the benefit for relapsed acute myeloid leukaemia (AML) and myelodisplastic syndrome (MDS) is often limited because of its rapid growth.
Aims
Analysis of patients with myeloid malignancies (including AML, MDS and secondary myelofibrosis) receiving RIC allo-HSCT with or without complete response (CR) in terms of transplant related mortality (TRM), event free survival (EFS) and overall survival (OS) in order to investigate the GVT in both groups.
Methods
We analysed 169 patients who underwent to allo-HSCT in our centre between 1995-2015. Characteristics of both groups are described on table 1. Although cytogenetic abnormalities are not available at this moment, the data is been recording and this variable will be included in the final analysis.
Results
In the overall series and with a median follow-up of 36 months for patients alive, the estimated OS and EFS at one year, two years and five years was 71%, 64% and 58% and 61%, 51% and 45% respectively. The mainly cause of death was relapse in 32 patients (19%) and 25 (15%) due to TRM. In the Kaplan-Meier analysis the variables associated with OS (p<0,05) were: CR status, III-IV acute graft versus host disease (GVHD), development of cGVHD, fungal infection, thrombotic microangiopathy and veno-occlussive disease while just the development of cGVHD (p=0,001) with differences between grades: limited (p=0,046, HR 0,37, 0,14-0,98) and extensive (p=0,00, HR 0,24, 0,11- 0,52) and development of thrombotic microangiopathy (p=0,004, HR 4,6, 1,6-12,8), but not CR status at the moment of allo-HSCT (p=0,49), maintained significance in multivariate analysis.Regarding the outcomes on the basis of disease status at transplant, there were differences between CR and not CR patients in terms of OS (p=0,02, not achieved vs 32 months) and EFS (p=0,012; 71 Vs 9 months) but there where no differences in PFS (p=0,6); attending the TRM (p=0,05, estimated 8% Vs 22% at 1 year), there were differences manly due to the GVHD related mortality (p=0,05; 2% Vs 17% at 1 year). Exploring the GVT in both groups separately: in the group of patients with CR, there were differences between patients without cGVHD compared with patients with limited or extensive cGVHD (p=0,00) with median OS not achieved in all groups; but in those patients without CR, just extensive cGVHD seems to be effective (p = 0,00) with a median OS not achieved Vs 10 and 28 months in those patients without and with limited cGVHD respectively.
Conclusion
In our series, the PFS of patients without CR at the moment of transplant was similar to those with CR, but the first group had worse OS, EFS and higher TRM due to a larger rate of severe acute GVHD with a high proportion of induced GVHD because the early withdrawal of the immunosuppressive treatment. On the other hand, patients without CR and development of extensive cGVHD had long term survival rates, similar to those patients with CR, reflecting the GVT. Efforts should be focus on avoid severe aGVHD maintaining the GVT in order to improve the TRM rates with new immunosuppressive strategies and improve the management of minimal residual disease.
Session topic: E-poster
Keyword(s): Acute myeloid leukemia, Graft-versus-tumor effect, Myelodysplasia, Reduced intensity transplantation
Type: Eposter Presentation
Background
Allo-transplant (allo-HSCT) has become a significant treatment for refractory and relapsed haematological malignances; however, relapse remains a mayor cause of treatment failure. Reduce intensity conditioning (RIC) regimens have shown to be safe and effective in older patients or with comorbidities, but patients with chemorefractory disease still have high relapse rates and poor outcomes. Although graft versus tumor effect (GVT) has been demonstrated in some malignancies, the benefit for relapsed acute myeloid leukaemia (AML) and myelodisplastic syndrome (MDS) is often limited because of its rapid growth.
Aims
Analysis of patients with myeloid malignancies (including AML, MDS and secondary myelofibrosis) receiving RIC allo-HSCT with or without complete response (CR) in terms of transplant related mortality (TRM), event free survival (EFS) and overall survival (OS) in order to investigate the GVT in both groups.
Methods
We analysed 169 patients who underwent to allo-HSCT in our centre between 1995-2015. Characteristics of both groups are described on table 1. Although cytogenetic abnormalities are not available at this moment, the data is been recording and this variable will be included in the final analysis.
Results
In the overall series and with a median follow-up of 36 months for patients alive, the estimated OS and EFS at one year, two years and five years was 71%, 64% and 58% and 61%, 51% and 45% respectively. The mainly cause of death was relapse in 32 patients (19%) and 25 (15%) due to TRM. In the Kaplan-Meier analysis the variables associated with OS (p<0,05) were: CR status, III-IV acute graft versus host disease (GVHD), development of cGVHD, fungal infection, thrombotic microangiopathy and veno-occlussive disease while just the development of cGVHD (p=0,001) with differences between grades: limited (p=0,046, HR 0,37, 0,14-0,98) and extensive (p=0,00, HR 0,24, 0,11- 0,52) and development of thrombotic microangiopathy (p=0,004, HR 4,6, 1,6-12,8), but not CR status at the moment of allo-HSCT (p=0,49), maintained significance in multivariate analysis.Regarding the outcomes on the basis of disease status at transplant, there were differences between CR and not CR patients in terms of OS (p=0,02, not achieved vs 32 months) and EFS (p=0,012; 71 Vs 9 months) but there where no differences in PFS (p=0,6); attending the TRM (p=0,05, estimated 8% Vs 22% at 1 year), there were differences manly due to the GVHD related mortality (p=0,05; 2% Vs 17% at 1 year). Exploring the GVT in both groups separately: in the group of patients with CR, there were differences between patients without cGVHD compared with patients with limited or extensive cGVHD (p=0,00) with median OS not achieved in all groups; but in those patients without CR, just extensive cGVHD seems to be effective (p = 0,00) with a median OS not achieved Vs 10 and 28 months in those patients without and with limited cGVHD respectively.
Conclusion
In our series, the PFS of patients without CR at the moment of transplant was similar to those with CR, but the first group had worse OS, EFS and higher TRM due to a larger rate of severe acute GVHD with a high proportion of induced GVHD because the early withdrawal of the immunosuppressive treatment. On the other hand, patients without CR and development of extensive cGVHD had long term survival rates, similar to those patients with CR, reflecting the GVT. Efforts should be focus on avoid severe aGVHD maintaining the GVT in order to improve the TRM rates with new immunosuppressive strategies and improve the management of minimal residual disease.
Session topic: E-poster
Keyword(s): Acute myeloid leukemia, Graft-versus-tumor effect, Myelodysplasia, Reduced intensity transplantation
{{ help_message }}
{{filter}}