
ICU AND LONG-TERM MORTALITY ANALISIS OF HEMATOLOGOGICAL MALIGNANCIES ADMITTED IN ICU. A UNICENTRIC SEVEN YEARS REVIEW IN A SPANISH HOSPITAL
(Abstract release date: 05/19/16)
EHA Library. Jiménez-Ubieto A. 06/09/16; 132995; E1446

Prof. Dr. Ana Jiménez-Ubieto
Contributions
Contributions
Abstract
Abstract: E1446
Type: Eposter Presentation
Background
Improvements in survival in patients with haematological malignancies (HM) admitted to the intensive care unit (ICU) has largely been reported in uncontrolled cohorts. Newly diagnosed patients should be admitted, since their prognosis is still to be defined. Nevertheless the admission of the remaining patients remains a matter of substantial controversy.
Aims
To analyse the survival of HM patients admitted to ICU over a 7-year period (from 2008 to 2014) in a single high complexity Spanish hospital
Methods
We conducted a detailed retrospective study of sequential adult ICU admissions with HM in a single centre, considering numerous variables with regard to their influence on ICU and mortality. Overall survival (OS) was defined as the time from ICU admission to death from any cause, and surviving patients were censored at last follow-up. OS were calculated using the Kaplan–Meier method estimates and the differences assessed by the log-rank test. All P-value less than 0.05 were considered significant.
Results
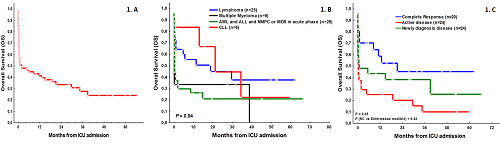
Overall, 67 HM patients were included, 62% were male, with a median age of 59 years (IQR: 19–82). The median APACHE II was 22 (IQR: 12-49). The hematologic diagnosis was as follow: 25 lymphomas (37%), 9 Multiple Myeloma (MM) (13%), 6 chronic lymphocytic leukaemia (CLL) (9%) and 28 acute leukaemia or myeloproliferative or myelodisplasic syndromes in acute phase (41%). Disease status at the moment of UCI admission was: 19 (28%) in complete response (CR), 24 (36%) with a newly diagnosis disease and 24 (36%) whit active disease (of those, 18 patients were refractory to disease specific treatment and 6 patients were chemosensitive). 67% of patients were on active oncologic treatment at the moment of UCI admission. Principal ICU diagnosis was sepsis (68%). Median number of organ failures was 2 (IQR: 0-4); 71% presented a respiratory and 70% a hemodynamic failure.70% accurate vasoactive drugs, 64% invasive mechanical ventilation and 34% dialysis. More than one third of patients (36%) presented neutropenia at the moment of UCI admission. Median ICU length of stay was 7 days (IQR: 1-48) and median hospital length of stay was 38 days (IQR: 8-109). ICU mortality was 46% (25% of the deaths occurred the first day of ICU admission, and 75% within the first week). The rates for ICU, 1-month, 6-month and 12 month mortality were 48%, 55% and 66%, respectively. With a median follow-up from the day of UCI admission of 18.5 months (IQR: 8-66), estimated OS at 1, 6 and 12 months were 51%, 44% and 41%, respectively (fig. 1a).Hematologic diagnosis (fig. 1b) status of the disease at the moment of ICU admission (fig. 1c) and the number of organ failure (≤ 2: 67% vs ≥ 3: 28%, P=.009) were the most powerful predictor variables associated with an increased OS.
Conclusion
OS of our HM patients is not worse than that recently reported from other specialist units.The decision for or against ICU admission of patients with HM should become dependent of the underlying malignant disease and especially with the status of the disease at the moment of admission. Almost 50% of survivors are still alive one year after ICU admission, suggesting that an important subgroup of HM patients benefit from ICU admission. In addition, only 25% of patients died beyond the 1st week of admission, not consuming resources without benefit. A multidisciplinary approach between intensivists and hematologists is essential in these patients.
Session topic: E-poster
Keyword(s): Chemosensitivity, Follow-up, Hematological malignancy, Survival
Type: Eposter Presentation
Background
Improvements in survival in patients with haematological malignancies (HM) admitted to the intensive care unit (ICU) has largely been reported in uncontrolled cohorts. Newly diagnosed patients should be admitted, since their prognosis is still to be defined. Nevertheless the admission of the remaining patients remains a matter of substantial controversy.
Aims
To analyse the survival of HM patients admitted to ICU over a 7-year period (from 2008 to 2014) in a single high complexity Spanish hospital
Methods
We conducted a detailed retrospective study of sequential adult ICU admissions with HM in a single centre, considering numerous variables with regard to their influence on ICU and mortality. Overall survival (OS) was defined as the time from ICU admission to death from any cause, and surviving patients were censored at last follow-up. OS were calculated using the Kaplan–Meier method estimates and the differences assessed by the log-rank test. All P-value less than 0.05 were considered significant.
Results
Overall, 67 HM patients were included, 62% were male, with a median age of 59 years (IQR: 19–82). The median APACHE II was 22 (IQR: 12-49). The hematologic diagnosis was as follow: 25 lymphomas (37%), 9 Multiple Myeloma (MM) (13%), 6 chronic lymphocytic leukaemia (CLL) (9%) and 28 acute leukaemia or myeloproliferative or myelodisplasic syndromes in acute phase (41%). Disease status at the moment of UCI admission was: 19 (28%) in complete response (CR), 24 (36%) with a newly diagnosis disease and 24 (36%) whit active disease (of those, 18 patients were refractory to disease specific treatment and 6 patients were chemosensitive). 67% of patients were on active oncologic treatment at the moment of UCI admission. Principal ICU diagnosis was sepsis (68%). Median number of organ failures was 2 (IQR: 0-4); 71% presented a respiratory and 70% a hemodynamic failure.70% accurate vasoactive drugs, 64% invasive mechanical ventilation and 34% dialysis. More than one third of patients (36%) presented neutropenia at the moment of UCI admission. Median ICU length of stay was 7 days (IQR: 1-48) and median hospital length of stay was 38 days (IQR: 8-109). ICU mortality was 46% (25% of the deaths occurred the first day of ICU admission, and 75% within the first week). The rates for ICU, 1-month, 6-month and 12 month mortality were 48%, 55% and 66%, respectively. With a median follow-up from the day of UCI admission of 18.5 months (IQR: 8-66), estimated OS at 1, 6 and 12 months were 51%, 44% and 41%, respectively (fig. 1a).Hematologic diagnosis (fig. 1b) status of the disease at the moment of ICU admission (fig. 1c) and the number of organ failure (≤ 2: 67% vs ≥ 3: 28%, P=.009) were the most powerful predictor variables associated with an increased OS.
Conclusion
OS of our HM patients is not worse than that recently reported from other specialist units.The decision for or against ICU admission of patients with HM should become dependent of the underlying malignant disease and especially with the status of the disease at the moment of admission. Almost 50% of survivors are still alive one year after ICU admission, suggesting that an important subgroup of HM patients benefit from ICU admission. In addition, only 25% of patients died beyond the 1st week of admission, not consuming resources without benefit. A multidisciplinary approach between intensivists and hematologists is essential in these patients.
Session topic: E-poster
Keyword(s): Chemosensitivity, Follow-up, Hematological malignancy, Survival
Abstract: E1446
Type: Eposter Presentation
Background
Improvements in survival in patients with haematological malignancies (HM) admitted to the intensive care unit (ICU) has largely been reported in uncontrolled cohorts. Newly diagnosed patients should be admitted, since their prognosis is still to be defined. Nevertheless the admission of the remaining patients remains a matter of substantial controversy.
Aims
To analyse the survival of HM patients admitted to ICU over a 7-year period (from 2008 to 2014) in a single high complexity Spanish hospital
Methods
We conducted a detailed retrospective study of sequential adult ICU admissions with HM in a single centre, considering numerous variables with regard to their influence on ICU and mortality. Overall survival (OS) was defined as the time from ICU admission to death from any cause, and surviving patients were censored at last follow-up. OS were calculated using the Kaplan–Meier method estimates and the differences assessed by the log-rank test. All P-value less than 0.05 were considered significant.
Results
Overall, 67 HM patients were included, 62% were male, with a median age of 59 years (IQR: 19–82). The median APACHE II was 22 (IQR: 12-49). The hematologic diagnosis was as follow: 25 lymphomas (37%), 9 Multiple Myeloma (MM) (13%), 6 chronic lymphocytic leukaemia (CLL) (9%) and 28 acute leukaemia or myeloproliferative or myelodisplasic syndromes in acute phase (41%). Disease status at the moment of UCI admission was: 19 (28%) in complete response (CR), 24 (36%) with a newly diagnosis disease and 24 (36%) whit active disease (of those, 18 patients were refractory to disease specific treatment and 6 patients were chemosensitive). 67% of patients were on active oncologic treatment at the moment of UCI admission. Principal ICU diagnosis was sepsis (68%). Median number of organ failures was 2 (IQR: 0-4); 71% presented a respiratory and 70% a hemodynamic failure.70% accurate vasoactive drugs, 64% invasive mechanical ventilation and 34% dialysis. More than one third of patients (36%) presented neutropenia at the moment of UCI admission. Median ICU length of stay was 7 days (IQR: 1-48) and median hospital length of stay was 38 days (IQR: 8-109). ICU mortality was 46% (25% of the deaths occurred the first day of ICU admission, and 75% within the first week). The rates for ICU, 1-month, 6-month and 12 month mortality were 48%, 55% and 66%, respectively. With a median follow-up from the day of UCI admission of 18.5 months (IQR: 8-66), estimated OS at 1, 6 and 12 months were 51%, 44% and 41%, respectively (fig. 1a).Hematologic diagnosis (fig. 1b) status of the disease at the moment of ICU admission (fig. 1c) and the number of organ failure (≤ 2: 67% vs ≥ 3: 28%, P=.009) were the most powerful predictor variables associated with an increased OS.
Conclusion
OS of our HM patients is not worse than that recently reported from other specialist units.The decision for or against ICU admission of patients with HM should become dependent of the underlying malignant disease and especially with the status of the disease at the moment of admission. Almost 50% of survivors are still alive one year after ICU admission, suggesting that an important subgroup of HM patients benefit from ICU admission. In addition, only 25% of patients died beyond the 1st week of admission, not consuming resources without benefit. A multidisciplinary approach between intensivists and hematologists is essential in these patients.
Session topic: E-poster
Keyword(s): Chemosensitivity, Follow-up, Hematological malignancy, Survival
Type: Eposter Presentation
Background
Improvements in survival in patients with haematological malignancies (HM) admitted to the intensive care unit (ICU) has largely been reported in uncontrolled cohorts. Newly diagnosed patients should be admitted, since their prognosis is still to be defined. Nevertheless the admission of the remaining patients remains a matter of substantial controversy.
Aims
To analyse the survival of HM patients admitted to ICU over a 7-year period (from 2008 to 2014) in a single high complexity Spanish hospital
Methods
We conducted a detailed retrospective study of sequential adult ICU admissions with HM in a single centre, considering numerous variables with regard to their influence on ICU and mortality. Overall survival (OS) was defined as the time from ICU admission to death from any cause, and surviving patients were censored at last follow-up. OS were calculated using the Kaplan–Meier method estimates and the differences assessed by the log-rank test. All P-value less than 0.05 were considered significant.
Results
Overall, 67 HM patients were included, 62% were male, with a median age of 59 years (IQR: 19–82). The median APACHE II was 22 (IQR: 12-49). The hematologic diagnosis was as follow: 25 lymphomas (37%), 9 Multiple Myeloma (MM) (13%), 6 chronic lymphocytic leukaemia (CLL) (9%) and 28 acute leukaemia or myeloproliferative or myelodisplasic syndromes in acute phase (41%). Disease status at the moment of UCI admission was: 19 (28%) in complete response (CR), 24 (36%) with a newly diagnosis disease and 24 (36%) whit active disease (of those, 18 patients were refractory to disease specific treatment and 6 patients were chemosensitive). 67% of patients were on active oncologic treatment at the moment of UCI admission. Principal ICU diagnosis was sepsis (68%). Median number of organ failures was 2 (IQR: 0-4); 71% presented a respiratory and 70% a hemodynamic failure.70% accurate vasoactive drugs, 64% invasive mechanical ventilation and 34% dialysis. More than one third of patients (36%) presented neutropenia at the moment of UCI admission. Median ICU length of stay was 7 days (IQR: 1-48) and median hospital length of stay was 38 days (IQR: 8-109). ICU mortality was 46% (25% of the deaths occurred the first day of ICU admission, and 75% within the first week). The rates for ICU, 1-month, 6-month and 12 month mortality were 48%, 55% and 66%, respectively. With a median follow-up from the day of UCI admission of 18.5 months (IQR: 8-66), estimated OS at 1, 6 and 12 months were 51%, 44% and 41%, respectively (fig. 1a).Hematologic diagnosis (fig. 1b) status of the disease at the moment of ICU admission (fig. 1c) and the number of organ failure (≤ 2: 67% vs ≥ 3: 28%, P=.009) were the most powerful predictor variables associated with an increased OS.
Conclusion
OS of our HM patients is not worse than that recently reported from other specialist units.The decision for or against ICU admission of patients with HM should become dependent of the underlying malignant disease and especially with the status of the disease at the moment of admission. Almost 50% of survivors are still alive one year after ICU admission, suggesting that an important subgroup of HM patients benefit from ICU admission. In addition, only 25% of patients died beyond the 1st week of admission, not consuming resources without benefit. A multidisciplinary approach between intensivists and hematologists is essential in these patients.
Session topic: E-poster
Keyword(s): Chemosensitivity, Follow-up, Hematological malignancy, Survival
{{ help_message }}
{{filter}}