
USEFULNESS OF PERFORMING JAK2 MUTATIONAL ANALYSIS IN PATIENTS WITH MODERATE ABSOLUTE ERYTHROCYTOSIS
(Abstract release date: 05/19/16)
EHA Library. Roncoroni E. 06/09/16; 132914; E1365

Dr. Elisa Roncoroni
Contributions
Contributions
Abstract
Abstract: E1365
Type: Eposter Presentation
Background
The diagnosis of polycythemia vera (PV) is based on clinical and biological criteria defined by the World Health Organization (WHO 2008). The proposed revised version (WHO 2016) has lowered the threshold hemoglobin (Hb) level for the diagnosis of PV from 18.5 g/dl in men and 16.5 g/dl in women to an hemoglobin level of 16.5 g/dl in men and 16 g/dl for women. The importance to lower hemoglobin threshold in the evaluation of patients with absolute erythrocytosis has not been validated yet.
Aims
To evaluate the importance of the new hemoglobin threshold we retrospectively assessed the frequency of polycythemia vera versus secondary erythrocytosis in patients with absolute erythrocytosis categorized according to hemoglobin value at diagnosis.
Methods
We included in the current study all patients recorded in our database with a diagnosis of polycythemia vera or secondary erythrocytosis who showed isolated absolute erythrocytosis at diagnosis according to the new proposed WHO criteria (Hb > 16.5 g/dl in men and > 16 g/dl in women, leukocyte count < 10 x109/L, platelet count < 450 x109/L). We stratified these patients according to their hemoglobin level at diagnosis (< 17 g/dl, 17-19 g/dl, 19-21 g/dl, 21-23 g/dl, >/= 23 g/dl) and calculated the percentage of PV cases in each subgroup. Only patients assessed for both V617F and exon 12 JAK2 mutations were included in the study.
Results
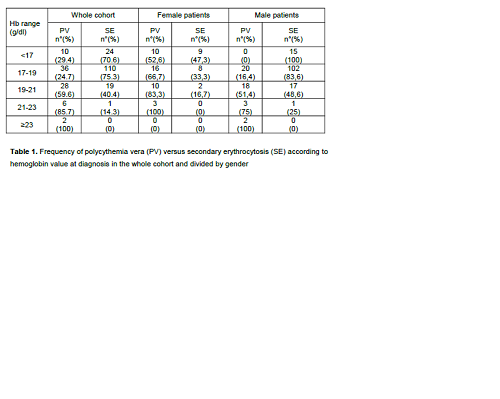
Patients who satisfied the above criteria were 236 patients, including 82 PV and 154 secondary erythrocytosis. Diagnosis of PV was made according to WHO 2008 criteria (Hb > 16,5 g/dl (female) or 18,5 g/dl (male) or > 15 g/dl (female) or 17 g/dl with a sustained increase of > 2 g/dl from baseline, JAK2 V617F or exon 12 mutation, low erythropoietin level and/or panmyelosis at bone marrow analysis). As shown in table 1, around one third of patients stratified in the subgroup with the lowest hemoglobin (Hb below 17 g/dl) had a final diagnosis of PV, thus reinforcing the importance to perform JAK2 analysis also in patients with moderate erythrocytosis. This was particularly important in female patients. Namely, when we repeated the same stratification taking into account sex distribution, we observed that half (52.6%) of female patients with Hb level < 17 g/dl received a final diagnosis of PV. According to our data set, instead, no male patient with Hb lower than 17 g/dl was diagnosed with polycythemia vera. Patients who satisfied the above criteria were 236 patients, including 82 PV and 154 secondary erythrocytosis. Diagnosis of PV was made according to WHO 2008 criteria (Hb > 16,5 g/dl (female) or 18,5 g/dl (male) or > 15 g/dl (female) or 17 g/dl with a sustained increase of > 2 g/dl from baseline, JAK2 V617F or exon 12 mutation, low erythropoietin level and/or panmyelosis at bone marrow analysis). As shown in table 1, around one third of patients stratified in the subgroup with the lowest hemoglobin (Hb below 17 g/dl) had a final diagnosis of PV, thus reinforcing the importance to perform JAK2 analysis also in patients with moderate erythrocytosis. This was particularly important in female patients. Namely, when we repeated the same stratification taking into account sex distribution, we observed that half (52.6%) of female patients with Hb level < 17 g/dl received a final diagnosis of PV. According to our data set, instead, no male patient with Hb lower than 17 g/dl was diagnosed with polycythemia vera.
Conclusion
In patients with isolate erythrocytosis it is important to perform screening for JAK2 mutations also when hemoglobin level is slightly increased (>16,5 in men and >16 in women) as a significative proportion of patients with polycythemia vera show at diagnosis only mild erythrocytosis. This result reinforces the importance to lower the hemoglobin threshold required for PV diagnosis as proposed by the new WHO criteria, especially as far as female patients are concerned.
Session topic: E-poster
Keyword(s): Erythrocytosis, Hemoglobin, Polycythemia vera
Type: Eposter Presentation
Background
The diagnosis of polycythemia vera (PV) is based on clinical and biological criteria defined by the World Health Organization (WHO 2008). The proposed revised version (WHO 2016) has lowered the threshold hemoglobin (Hb) level for the diagnosis of PV from 18.5 g/dl in men and 16.5 g/dl in women to an hemoglobin level of 16.5 g/dl in men and 16 g/dl for women. The importance to lower hemoglobin threshold in the evaluation of patients with absolute erythrocytosis has not been validated yet.
Aims
To evaluate the importance of the new hemoglobin threshold we retrospectively assessed the frequency of polycythemia vera versus secondary erythrocytosis in patients with absolute erythrocytosis categorized according to hemoglobin value at diagnosis.
Methods
We included in the current study all patients recorded in our database with a diagnosis of polycythemia vera or secondary erythrocytosis who showed isolated absolute erythrocytosis at diagnosis according to the new proposed WHO criteria (Hb > 16.5 g/dl in men and > 16 g/dl in women, leukocyte count < 10 x109/L, platelet count < 450 x109/L). We stratified these patients according to their hemoglobin level at diagnosis (< 17 g/dl, 17-19 g/dl, 19-21 g/dl, 21-23 g/dl, >/= 23 g/dl) and calculated the percentage of PV cases in each subgroup. Only patients assessed for both V617F and exon 12 JAK2 mutations were included in the study.
Results
Patients who satisfied the above criteria were 236 patients, including 82 PV and 154 secondary erythrocytosis. Diagnosis of PV was made according to WHO 2008 criteria (Hb > 16,5 g/dl (female) or 18,5 g/dl (male) or > 15 g/dl (female) or 17 g/dl with a sustained increase of > 2 g/dl from baseline, JAK2 V617F or exon 12 mutation, low erythropoietin level and/or panmyelosis at bone marrow analysis). As shown in table 1, around one third of patients stratified in the subgroup with the lowest hemoglobin (Hb below 17 g/dl) had a final diagnosis of PV, thus reinforcing the importance to perform JAK2 analysis also in patients with moderate erythrocytosis. This was particularly important in female patients. Namely, when we repeated the same stratification taking into account sex distribution, we observed that half (52.6%) of female patients with Hb level < 17 g/dl received a final diagnosis of PV. According to our data set, instead, no male patient with Hb lower than 17 g/dl was diagnosed with polycythemia vera. Patients who satisfied the above criteria were 236 patients, including 82 PV and 154 secondary erythrocytosis. Diagnosis of PV was made according to WHO 2008 criteria (Hb > 16,5 g/dl (female) or 18,5 g/dl (male) or > 15 g/dl (female) or 17 g/dl with a sustained increase of > 2 g/dl from baseline, JAK2 V617F or exon 12 mutation, low erythropoietin level and/or panmyelosis at bone marrow analysis). As shown in table 1, around one third of patients stratified in the subgroup with the lowest hemoglobin (Hb below 17 g/dl) had a final diagnosis of PV, thus reinforcing the importance to perform JAK2 analysis also in patients with moderate erythrocytosis. This was particularly important in female patients. Namely, when we repeated the same stratification taking into account sex distribution, we observed that half (52.6%) of female patients with Hb level < 17 g/dl received a final diagnosis of PV. According to our data set, instead, no male patient with Hb lower than 17 g/dl was diagnosed with polycythemia vera.
Conclusion
In patients with isolate erythrocytosis it is important to perform screening for JAK2 mutations also when hemoglobin level is slightly increased (>16,5 in men and >16 in women) as a significative proportion of patients with polycythemia vera show at diagnosis only mild erythrocytosis. This result reinforces the importance to lower the hemoglobin threshold required for PV diagnosis as proposed by the new WHO criteria, especially as far as female patients are concerned.
Session topic: E-poster
Keyword(s): Erythrocytosis, Hemoglobin, Polycythemia vera
Abstract: E1365
Type: Eposter Presentation
Background
The diagnosis of polycythemia vera (PV) is based on clinical and biological criteria defined by the World Health Organization (WHO 2008). The proposed revised version (WHO 2016) has lowered the threshold hemoglobin (Hb) level for the diagnosis of PV from 18.5 g/dl in men and 16.5 g/dl in women to an hemoglobin level of 16.5 g/dl in men and 16 g/dl for women. The importance to lower hemoglobin threshold in the evaluation of patients with absolute erythrocytosis has not been validated yet.
Aims
To evaluate the importance of the new hemoglobin threshold we retrospectively assessed the frequency of polycythemia vera versus secondary erythrocytosis in patients with absolute erythrocytosis categorized according to hemoglobin value at diagnosis.
Methods
We included in the current study all patients recorded in our database with a diagnosis of polycythemia vera or secondary erythrocytosis who showed isolated absolute erythrocytosis at diagnosis according to the new proposed WHO criteria (Hb > 16.5 g/dl in men and > 16 g/dl in women, leukocyte count < 10 x109/L, platelet count < 450 x109/L). We stratified these patients according to their hemoglobin level at diagnosis (< 17 g/dl, 17-19 g/dl, 19-21 g/dl, 21-23 g/dl, >/= 23 g/dl) and calculated the percentage of PV cases in each subgroup. Only patients assessed for both V617F and exon 12 JAK2 mutations were included in the study.
Results
Patients who satisfied the above criteria were 236 patients, including 82 PV and 154 secondary erythrocytosis. Diagnosis of PV was made according to WHO 2008 criteria (Hb > 16,5 g/dl (female) or 18,5 g/dl (male) or > 15 g/dl (female) or 17 g/dl with a sustained increase of > 2 g/dl from baseline, JAK2 V617F or exon 12 mutation, low erythropoietin level and/or panmyelosis at bone marrow analysis). As shown in table 1, around one third of patients stratified in the subgroup with the lowest hemoglobin (Hb below 17 g/dl) had a final diagnosis of PV, thus reinforcing the importance to perform JAK2 analysis also in patients with moderate erythrocytosis. This was particularly important in female patients. Namely, when we repeated the same stratification taking into account sex distribution, we observed that half (52.6%) of female patients with Hb level < 17 g/dl received a final diagnosis of PV. According to our data set, instead, no male patient with Hb lower than 17 g/dl was diagnosed with polycythemia vera. Patients who satisfied the above criteria were 236 patients, including 82 PV and 154 secondary erythrocytosis. Diagnosis of PV was made according to WHO 2008 criteria (Hb > 16,5 g/dl (female) or 18,5 g/dl (male) or > 15 g/dl (female) or 17 g/dl with a sustained increase of > 2 g/dl from baseline, JAK2 V617F or exon 12 mutation, low erythropoietin level and/or panmyelosis at bone marrow analysis). As shown in table 1, around one third of patients stratified in the subgroup with the lowest hemoglobin (Hb below 17 g/dl) had a final diagnosis of PV, thus reinforcing the importance to perform JAK2 analysis also in patients with moderate erythrocytosis. This was particularly important in female patients. Namely, when we repeated the same stratification taking into account sex distribution, we observed that half (52.6%) of female patients with Hb level < 17 g/dl received a final diagnosis of PV. According to our data set, instead, no male patient with Hb lower than 17 g/dl was diagnosed with polycythemia vera.
Conclusion
In patients with isolate erythrocytosis it is important to perform screening for JAK2 mutations also when hemoglobin level is slightly increased (>16,5 in men and >16 in women) as a significative proportion of patients with polycythemia vera show at diagnosis only mild erythrocytosis. This result reinforces the importance to lower the hemoglobin threshold required for PV diagnosis as proposed by the new WHO criteria, especially as far as female patients are concerned.
Session topic: E-poster
Keyword(s): Erythrocytosis, Hemoglobin, Polycythemia vera
Type: Eposter Presentation
Background
The diagnosis of polycythemia vera (PV) is based on clinical and biological criteria defined by the World Health Organization (WHO 2008). The proposed revised version (WHO 2016) has lowered the threshold hemoglobin (Hb) level for the diagnosis of PV from 18.5 g/dl in men and 16.5 g/dl in women to an hemoglobin level of 16.5 g/dl in men and 16 g/dl for women. The importance to lower hemoglobin threshold in the evaluation of patients with absolute erythrocytosis has not been validated yet.
Aims
To evaluate the importance of the new hemoglobin threshold we retrospectively assessed the frequency of polycythemia vera versus secondary erythrocytosis in patients with absolute erythrocytosis categorized according to hemoglobin value at diagnosis.
Methods
We included in the current study all patients recorded in our database with a diagnosis of polycythemia vera or secondary erythrocytosis who showed isolated absolute erythrocytosis at diagnosis according to the new proposed WHO criteria (Hb > 16.5 g/dl in men and > 16 g/dl in women, leukocyte count < 10 x109/L, platelet count < 450 x109/L). We stratified these patients according to their hemoglobin level at diagnosis (< 17 g/dl, 17-19 g/dl, 19-21 g/dl, 21-23 g/dl, >/= 23 g/dl) and calculated the percentage of PV cases in each subgroup. Only patients assessed for both V617F and exon 12 JAK2 mutations were included in the study.
Results
Patients who satisfied the above criteria were 236 patients, including 82 PV and 154 secondary erythrocytosis. Diagnosis of PV was made according to WHO 2008 criteria (Hb > 16,5 g/dl (female) or 18,5 g/dl (male) or > 15 g/dl (female) or 17 g/dl with a sustained increase of > 2 g/dl from baseline, JAK2 V617F or exon 12 mutation, low erythropoietin level and/or panmyelosis at bone marrow analysis). As shown in table 1, around one third of patients stratified in the subgroup with the lowest hemoglobin (Hb below 17 g/dl) had a final diagnosis of PV, thus reinforcing the importance to perform JAK2 analysis also in patients with moderate erythrocytosis. This was particularly important in female patients. Namely, when we repeated the same stratification taking into account sex distribution, we observed that half (52.6%) of female patients with Hb level < 17 g/dl received a final diagnosis of PV. According to our data set, instead, no male patient with Hb lower than 17 g/dl was diagnosed with polycythemia vera. Patients who satisfied the above criteria were 236 patients, including 82 PV and 154 secondary erythrocytosis. Diagnosis of PV was made according to WHO 2008 criteria (Hb > 16,5 g/dl (female) or 18,5 g/dl (male) or > 15 g/dl (female) or 17 g/dl with a sustained increase of > 2 g/dl from baseline, JAK2 V617F or exon 12 mutation, low erythropoietin level and/or panmyelosis at bone marrow analysis). As shown in table 1, around one third of patients stratified in the subgroup with the lowest hemoglobin (Hb below 17 g/dl) had a final diagnosis of PV, thus reinforcing the importance to perform JAK2 analysis also in patients with moderate erythrocytosis. This was particularly important in female patients. Namely, when we repeated the same stratification taking into account sex distribution, we observed that half (52.6%) of female patients with Hb level < 17 g/dl received a final diagnosis of PV. According to our data set, instead, no male patient with Hb lower than 17 g/dl was diagnosed with polycythemia vera.
Conclusion
In patients with isolate erythrocytosis it is important to perform screening for JAK2 mutations also when hemoglobin level is slightly increased (>16,5 in men and >16 in women) as a significative proportion of patients with polycythemia vera show at diagnosis only mild erythrocytosis. This result reinforces the importance to lower the hemoglobin threshold required for PV diagnosis as proposed by the new WHO criteria, especially as far as female patients are concerned.
Session topic: E-poster
Keyword(s): Erythrocytosis, Hemoglobin, Polycythemia vera
{{ help_message }}
{{filter}}