
THE FIRST TRIAL: ANALYSIS OF THE ASIAN SUBGROUP OF TRANSPLANT-INELIGIBLE PATIENTS WITH NEWLY DIAGNOSED MULTIPLE MYELOMA TREATED WITH CONTINUOUS LENALIDOMIDE AND LOW-DOSE DEXAMETHASONE
(Abstract release date: 05/19/16)
EHA Library. Lu J. 06/09/16; 132874; E1325

Prof. Dr. Jin Lu
Contributions
Contributions
Abstract
Abstract: E1325
Type: Eposter Presentation
Background
The incidence of multiple myeloma (MM) in Asian countries is increasing; therefore, effective treatment options for these patient (pt) populations are needed (Kim et al, Am J Hematol, 2014). The pivotal phase 3 FIRST trial investigated continuous treatment with lenalidomide plus low-dose dexamethasone until disease progression (Rd continuous) in pts with newly diagnosed MM (NDMM) who were ineligible for autologous stem cell transplant (ASCT) from 18 countries, including China, South Korea, and Taiwan. Treatment with Rd continuous in the FIRST trial improved progression-free survival (PFS; hazard ratio [HR] = 0.72; P < .001) and overall survival (OS; HR = 0.78; P = .02) compared with melphalan-prednisone-thalidomide (MPT) (Benboubker et al, N Engl J Med, 2014).
Aims
To examine the efficacy and safety of Rd continuous in the Asian population of the FIRST trial.
Methods
Pts with NDMM aged ≥ 65 years or ineligible for transplant were randomized to 3 treatment arms: Rd continuous, Rd for 18 cycles (Rd18; 72 weeks), or MPT for 12 cycles (72 weeks). The primary endpoint was PFS in pts treated with Rd continuous vs those treated with MPT (primary comparators). Data cutoff was May 24, 2013; response and progression were assessed by an independent response adjudication committee. Data cutoff for OS was extended to March 3, 2014. All pts provided informed written consent.
Results
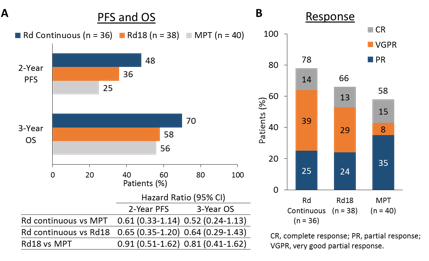
In the 114 pts enrolled in Asia, median age (68 yrs [range, 43-86 yrs]) was similar across the Rd continuous (n = 36), Rd18 (n = 38), and MPT (n = 40) arms but lower than that of the overall study population (73 yrs [range, 40-92 yrs]). Pts in Asia also had a higher rate of Eastern Cooperative Oncology Group performance status ≥ 2 (28% vs 22% overall), a higher rate of International Staging System stage III disease (45% vs 41% overall), and double the rate of severe renal insufficiency (creatinine clearance < 30 mL/min; 18% vs 9% overall), the latter of which was more frequent in the MPT (23%) and Rd18 (24%) arms vs the Rd continuous arm (8%). Median treatment duration was 18.4 mos (range, 0.5-35.9 mos) for Rd continuous, 11.0 mos (range, 0.6-19.6 mos) for Rd18, and 11.1 mos (range, 0.3-19.1 mos) for MPT. Treatment with Rd continuous vs MPT resulted in a 39% reduction in the risk of progression or death (Figure A). Rates of 2-year PFS were nearly doubled with Rd continuous (48%) vs MPT (25%). Rd continuous also resulted in a 48% reduced risk of death vs MPT. Overall response rate was greater in the Rd continuous arm (78%) vs the Rd18 (66%) and MPT (58%) arms (Figure B). Median duration of response was not reached for Rd continuous and was 17.2 and 13.8 mos for Rd18 and MPT, respectively. The most frequent grade 3/4 adverse events with Rd continuous, Rd18, and MPT were neutropenia (25%, 34%, 44%), anemia (19%, 5%, 15%), pneumonia (6%, 24%, 15%), and thrombocytopenia (14%, 5%, 5%). Deep vein thrombosis was reported in 1 pt in the MPT arm, and pulmonary embolism was reported in 1 pt in each treatment arm. There were no reports of second primary malignancies in the Asian population.
Conclusion
Rd continuous treatment resulted in numerically larger PFS and OS benefits and higher response rates compared with MPT in the Asian subgroup of the FIRST trial, although pt numbers were small. Results were consistent with those in the overall population, with no unexpected safety signals, a low rate of thromboembolic events, and no second primary malignancies as of data cutoff. These findings support Rd continuous as a standard treatment for pts with NDMM who are ineligible for ASCT, including Asian populations.
Session topic: E-poster
Type: Eposter Presentation
Background
The incidence of multiple myeloma (MM) in Asian countries is increasing; therefore, effective treatment options for these patient (pt) populations are needed (Kim et al, Am J Hematol, 2014). The pivotal phase 3 FIRST trial investigated continuous treatment with lenalidomide plus low-dose dexamethasone until disease progression (Rd continuous) in pts with newly diagnosed MM (NDMM) who were ineligible for autologous stem cell transplant (ASCT) from 18 countries, including China, South Korea, and Taiwan. Treatment with Rd continuous in the FIRST trial improved progression-free survival (PFS; hazard ratio [HR] = 0.72; P < .001) and overall survival (OS; HR = 0.78; P = .02) compared with melphalan-prednisone-thalidomide (MPT) (Benboubker et al, N Engl J Med, 2014).
Aims
To examine the efficacy and safety of Rd continuous in the Asian population of the FIRST trial.
Methods
Pts with NDMM aged ≥ 65 years or ineligible for transplant were randomized to 3 treatment arms: Rd continuous, Rd for 18 cycles (Rd18; 72 weeks), or MPT for 12 cycles (72 weeks). The primary endpoint was PFS in pts treated with Rd continuous vs those treated with MPT (primary comparators). Data cutoff was May 24, 2013; response and progression were assessed by an independent response adjudication committee. Data cutoff for OS was extended to March 3, 2014. All pts provided informed written consent.
Results
In the 114 pts enrolled in Asia, median age (68 yrs [range, 43-86 yrs]) was similar across the Rd continuous (n = 36), Rd18 (n = 38), and MPT (n = 40) arms but lower than that of the overall study population (73 yrs [range, 40-92 yrs]). Pts in Asia also had a higher rate of Eastern Cooperative Oncology Group performance status ≥ 2 (28% vs 22% overall), a higher rate of International Staging System stage III disease (45% vs 41% overall), and double the rate of severe renal insufficiency (creatinine clearance < 30 mL/min; 18% vs 9% overall), the latter of which was more frequent in the MPT (23%) and Rd18 (24%) arms vs the Rd continuous arm (8%). Median treatment duration was 18.4 mos (range, 0.5-35.9 mos) for Rd continuous, 11.0 mos (range, 0.6-19.6 mos) for Rd18, and 11.1 mos (range, 0.3-19.1 mos) for MPT. Treatment with Rd continuous vs MPT resulted in a 39% reduction in the risk of progression or death (Figure A). Rates of 2-year PFS were nearly doubled with Rd continuous (48%) vs MPT (25%). Rd continuous also resulted in a 48% reduced risk of death vs MPT. Overall response rate was greater in the Rd continuous arm (78%) vs the Rd18 (66%) and MPT (58%) arms (Figure B). Median duration of response was not reached for Rd continuous and was 17.2 and 13.8 mos for Rd18 and MPT, respectively. The most frequent grade 3/4 adverse events with Rd continuous, Rd18, and MPT were neutropenia (25%, 34%, 44%), anemia (19%, 5%, 15%), pneumonia (6%, 24%, 15%), and thrombocytopenia (14%, 5%, 5%). Deep vein thrombosis was reported in 1 pt in the MPT arm, and pulmonary embolism was reported in 1 pt in each treatment arm. There were no reports of second primary malignancies in the Asian population.
Conclusion
Rd continuous treatment resulted in numerically larger PFS and OS benefits and higher response rates compared with MPT in the Asian subgroup of the FIRST trial, although pt numbers were small. Results were consistent with those in the overall population, with no unexpected safety signals, a low rate of thromboembolic events, and no second primary malignancies as of data cutoff. These findings support Rd continuous as a standard treatment for pts with NDMM who are ineligible for ASCT, including Asian populations.
Session topic: E-poster
Abstract: E1325
Type: Eposter Presentation
Background
The incidence of multiple myeloma (MM) in Asian countries is increasing; therefore, effective treatment options for these patient (pt) populations are needed (Kim et al, Am J Hematol, 2014). The pivotal phase 3 FIRST trial investigated continuous treatment with lenalidomide plus low-dose dexamethasone until disease progression (Rd continuous) in pts with newly diagnosed MM (NDMM) who were ineligible for autologous stem cell transplant (ASCT) from 18 countries, including China, South Korea, and Taiwan. Treatment with Rd continuous in the FIRST trial improved progression-free survival (PFS; hazard ratio [HR] = 0.72; P < .001) and overall survival (OS; HR = 0.78; P = .02) compared with melphalan-prednisone-thalidomide (MPT) (Benboubker et al, N Engl J Med, 2014).
Aims
To examine the efficacy and safety of Rd continuous in the Asian population of the FIRST trial.
Methods
Pts with NDMM aged ≥ 65 years or ineligible for transplant were randomized to 3 treatment arms: Rd continuous, Rd for 18 cycles (Rd18; 72 weeks), or MPT for 12 cycles (72 weeks). The primary endpoint was PFS in pts treated with Rd continuous vs those treated with MPT (primary comparators). Data cutoff was May 24, 2013; response and progression were assessed by an independent response adjudication committee. Data cutoff for OS was extended to March 3, 2014. All pts provided informed written consent.
Results
In the 114 pts enrolled in Asia, median age (68 yrs [range, 43-86 yrs]) was similar across the Rd continuous (n = 36), Rd18 (n = 38), and MPT (n = 40) arms but lower than that of the overall study population (73 yrs [range, 40-92 yrs]). Pts in Asia also had a higher rate of Eastern Cooperative Oncology Group performance status ≥ 2 (28% vs 22% overall), a higher rate of International Staging System stage III disease (45% vs 41% overall), and double the rate of severe renal insufficiency (creatinine clearance < 30 mL/min; 18% vs 9% overall), the latter of which was more frequent in the MPT (23%) and Rd18 (24%) arms vs the Rd continuous arm (8%). Median treatment duration was 18.4 mos (range, 0.5-35.9 mos) for Rd continuous, 11.0 mos (range, 0.6-19.6 mos) for Rd18, and 11.1 mos (range, 0.3-19.1 mos) for MPT. Treatment with Rd continuous vs MPT resulted in a 39% reduction in the risk of progression or death (Figure A). Rates of 2-year PFS were nearly doubled with Rd continuous (48%) vs MPT (25%). Rd continuous also resulted in a 48% reduced risk of death vs MPT. Overall response rate was greater in the Rd continuous arm (78%) vs the Rd18 (66%) and MPT (58%) arms (Figure B). Median duration of response was not reached for Rd continuous and was 17.2 and 13.8 mos for Rd18 and MPT, respectively. The most frequent grade 3/4 adverse events with Rd continuous, Rd18, and MPT were neutropenia (25%, 34%, 44%), anemia (19%, 5%, 15%), pneumonia (6%, 24%, 15%), and thrombocytopenia (14%, 5%, 5%). Deep vein thrombosis was reported in 1 pt in the MPT arm, and pulmonary embolism was reported in 1 pt in each treatment arm. There were no reports of second primary malignancies in the Asian population.
Conclusion
Rd continuous treatment resulted in numerically larger PFS and OS benefits and higher response rates compared with MPT in the Asian subgroup of the FIRST trial, although pt numbers were small. Results were consistent with those in the overall population, with no unexpected safety signals, a low rate of thromboembolic events, and no second primary malignancies as of data cutoff. These findings support Rd continuous as a standard treatment for pts with NDMM who are ineligible for ASCT, including Asian populations.
Session topic: E-poster
Type: Eposter Presentation
Background
The incidence of multiple myeloma (MM) in Asian countries is increasing; therefore, effective treatment options for these patient (pt) populations are needed (Kim et al, Am J Hematol, 2014). The pivotal phase 3 FIRST trial investigated continuous treatment with lenalidomide plus low-dose dexamethasone until disease progression (Rd continuous) in pts with newly diagnosed MM (NDMM) who were ineligible for autologous stem cell transplant (ASCT) from 18 countries, including China, South Korea, and Taiwan. Treatment with Rd continuous in the FIRST trial improved progression-free survival (PFS; hazard ratio [HR] = 0.72; P < .001) and overall survival (OS; HR = 0.78; P = .02) compared with melphalan-prednisone-thalidomide (MPT) (Benboubker et al, N Engl J Med, 2014).
Aims
To examine the efficacy and safety of Rd continuous in the Asian population of the FIRST trial.
Methods
Pts with NDMM aged ≥ 65 years or ineligible for transplant were randomized to 3 treatment arms: Rd continuous, Rd for 18 cycles (Rd18; 72 weeks), or MPT for 12 cycles (72 weeks). The primary endpoint was PFS in pts treated with Rd continuous vs those treated with MPT (primary comparators). Data cutoff was May 24, 2013; response and progression were assessed by an independent response adjudication committee. Data cutoff for OS was extended to March 3, 2014. All pts provided informed written consent.
Results
In the 114 pts enrolled in Asia, median age (68 yrs [range, 43-86 yrs]) was similar across the Rd continuous (n = 36), Rd18 (n = 38), and MPT (n = 40) arms but lower than that of the overall study population (73 yrs [range, 40-92 yrs]). Pts in Asia also had a higher rate of Eastern Cooperative Oncology Group performance status ≥ 2 (28% vs 22% overall), a higher rate of International Staging System stage III disease (45% vs 41% overall), and double the rate of severe renal insufficiency (creatinine clearance < 30 mL/min; 18% vs 9% overall), the latter of which was more frequent in the MPT (23%) and Rd18 (24%) arms vs the Rd continuous arm (8%). Median treatment duration was 18.4 mos (range, 0.5-35.9 mos) for Rd continuous, 11.0 mos (range, 0.6-19.6 mos) for Rd18, and 11.1 mos (range, 0.3-19.1 mos) for MPT. Treatment with Rd continuous vs MPT resulted in a 39% reduction in the risk of progression or death (Figure A). Rates of 2-year PFS were nearly doubled with Rd continuous (48%) vs MPT (25%). Rd continuous also resulted in a 48% reduced risk of death vs MPT. Overall response rate was greater in the Rd continuous arm (78%) vs the Rd18 (66%) and MPT (58%) arms (Figure B). Median duration of response was not reached for Rd continuous and was 17.2 and 13.8 mos for Rd18 and MPT, respectively. The most frequent grade 3/4 adverse events with Rd continuous, Rd18, and MPT were neutropenia (25%, 34%, 44%), anemia (19%, 5%, 15%), pneumonia (6%, 24%, 15%), and thrombocytopenia (14%, 5%, 5%). Deep vein thrombosis was reported in 1 pt in the MPT arm, and pulmonary embolism was reported in 1 pt in each treatment arm. There were no reports of second primary malignancies in the Asian population.
Conclusion
Rd continuous treatment resulted in numerically larger PFS and OS benefits and higher response rates compared with MPT in the Asian subgroup of the FIRST trial, although pt numbers were small. Results were consistent with those in the overall population, with no unexpected safety signals, a low rate of thromboembolic events, and no second primary malignancies as of data cutoff. These findings support Rd continuous as a standard treatment for pts with NDMM who are ineligible for ASCT, including Asian populations.
Session topic: E-poster
{{ help_message }}
{{filter}}