
COMPARISON OF PERIPHERAL BLOOD STEM CELL (PBSC) MOBILIZATION WITH G-CSF ALONE VS G-CSF WITH CYCLOPHOSPHAMIDE POST VCD INDUCTION IN MULTIPLE MYELOMA
(Abstract release date: 05/19/16)
EHA Library. Chua C. 06/09/16; 132857; E1308

Dr. Chong Chyn Chua
Contributions
Contributions
Abstract
Abstract: E1308
Type: Eposter Presentation
Background
Bortezomib, cyclophosphamide and dexamethasone (VCD) combination is often used as induction therapy in transplant eligible patients with multiple myeloma (MM). However, the optimal PBSC mobilization strategy in this context is not established.
Aims
To review the efficacy of G-CSF alone (G-alone) versus G-CSF and cyclophosphamide (G-cyclo) PBSC mobilization strategies in MM patients who had only received VCD induction prior to autograft.
Methods
Retrospective review of PBSC mobilization strategies in patients from six apheresis centres from November 2012 to March 2015 after receiving VCD induction. Extended data were collected from a single centre to January 2016. Prior radiotherapy was not an exclusion criterion. Successful mobilization was defined as achieving physician-determined target PBSC yield, which in some older patients was ≥2x106/kg but in most patients was ≥4x106/kg to allow for two autografts (≥90% of both groups). Plerixafor was used in some centres as a rescue strategy if PB CD34 ≤10x106/L on the day of planned collection or PBSC yield was <1x106/kg after first apheresis. Univariate analysis was performed using chi-squared test for categorical data and Mann-Whitney-U test for continuous variables.
Results
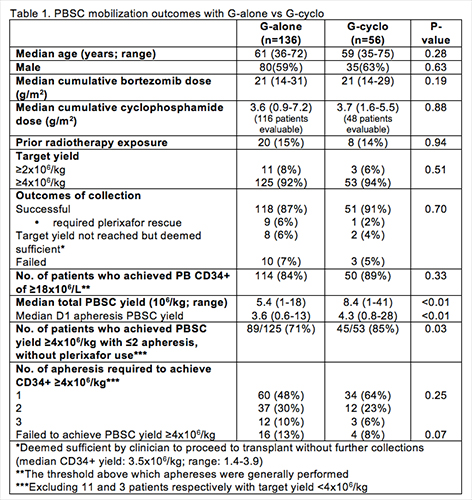
Table 1 summarizes the results of 192 patients. Baseline characteristics and cumulative exposure to bortezomib and cyclophosphamide were similar in both groups. G-alone strategy consisted of G-CSF at 10μg/kg/day (n=120) or 20μg/kg /day (n=16), administered for a median of 5 days. G-cyclo comprised of intravenous cyclophosphamide (1g/m2 (n=1), 1.5g/m2 (n=14), 2g/m2 (n=25), 3g/m2 (n=4), 4g/m2 (n=12)) with either G-CSF 5-10μg/kg/day for a median of 4 days (n=35) or single-dose 6mg pegfilgrastim (n=21). Overall, the rates of successful mobilization and the proportion of patients achieving a total PBSC yield of ≥4x106/kg were comparable between G-alone and G-cyclo with no significant difference in the median number of aphereses to reach this target. However the G-cyclo group had a significantly higher median PBSC yield per apheresis and a higher proportion of patients attaining a PBSC yield of ≥4x106/kg with ≤2 apheresis without rescue plerixafor. Ten (18%) G-cyclo patients had unplanned hospitalization, of which 8 had febrile neutropenia. In the G-alone group, age ≤60 and G-CSF doses of 20μg/d were significantly associated with a higher median PBSC yield. In the G-cyclo group, higher cyclophosphamide doses for mobilization (3-4g/m2 vs 1-2g/m2) resulted in a significantly higher PBSC yield. Cumulative bortezomib doses, pre-mobilization platelet count and prior radiotherapy did not significantly impact on PBSC yield in either group.
Conclusion
Despite a significantly higher PBSC yield with G-cyclo mobilization, the G-alone strategy is a reasonable first approach to mobilizing stem cells in the majority of patients receiving VCD induction.
Session topic: E-poster
Keyword(s): Bortezomib, Myeloma, Stem cell mobilization
Type: Eposter Presentation
Background
Bortezomib, cyclophosphamide and dexamethasone (VCD) combination is often used as induction therapy in transplant eligible patients with multiple myeloma (MM). However, the optimal PBSC mobilization strategy in this context is not established.
Aims
To review the efficacy of G-CSF alone (G-alone) versus G-CSF and cyclophosphamide (G-cyclo) PBSC mobilization strategies in MM patients who had only received VCD induction prior to autograft.
Methods
Retrospective review of PBSC mobilization strategies in patients from six apheresis centres from November 2012 to March 2015 after receiving VCD induction. Extended data were collected from a single centre to January 2016. Prior radiotherapy was not an exclusion criterion. Successful mobilization was defined as achieving physician-determined target PBSC yield, which in some older patients was ≥2x106/kg but in most patients was ≥4x106/kg to allow for two autografts (≥90% of both groups). Plerixafor was used in some centres as a rescue strategy if PB CD34 ≤10x106/L on the day of planned collection or PBSC yield was <1x106/kg after first apheresis. Univariate analysis was performed using chi-squared test for categorical data and Mann-Whitney-U test for continuous variables.
Results
Table 1 summarizes the results of 192 patients. Baseline characteristics and cumulative exposure to bortezomib and cyclophosphamide were similar in both groups. G-alone strategy consisted of G-CSF at 10μg/kg/day (n=120) or 20μg/kg /day (n=16), administered for a median of 5 days. G-cyclo comprised of intravenous cyclophosphamide (1g/m2 (n=1), 1.5g/m2 (n=14), 2g/m2 (n=25), 3g/m2 (n=4), 4g/m2 (n=12)) with either G-CSF 5-10μg/kg/day for a median of 4 days (n=35) or single-dose 6mg pegfilgrastim (n=21). Overall, the rates of successful mobilization and the proportion of patients achieving a total PBSC yield of ≥4x106/kg were comparable between G-alone and G-cyclo with no significant difference in the median number of aphereses to reach this target. However the G-cyclo group had a significantly higher median PBSC yield per apheresis and a higher proportion of patients attaining a PBSC yield of ≥4x106/kg with ≤2 apheresis without rescue plerixafor. Ten (18%) G-cyclo patients had unplanned hospitalization, of which 8 had febrile neutropenia. In the G-alone group, age ≤60 and G-CSF doses of 20μg/d were significantly associated with a higher median PBSC yield. In the G-cyclo group, higher cyclophosphamide doses for mobilization (3-4g/m2 vs 1-2g/m2) resulted in a significantly higher PBSC yield. Cumulative bortezomib doses, pre-mobilization platelet count and prior radiotherapy did not significantly impact on PBSC yield in either group.
Conclusion
Despite a significantly higher PBSC yield with G-cyclo mobilization, the G-alone strategy is a reasonable first approach to mobilizing stem cells in the majority of patients receiving VCD induction.
Session topic: E-poster
Keyword(s): Bortezomib, Myeloma, Stem cell mobilization
Abstract: E1308
Type: Eposter Presentation
Background
Bortezomib, cyclophosphamide and dexamethasone (VCD) combination is often used as induction therapy in transplant eligible patients with multiple myeloma (MM). However, the optimal PBSC mobilization strategy in this context is not established.
Aims
To review the efficacy of G-CSF alone (G-alone) versus G-CSF and cyclophosphamide (G-cyclo) PBSC mobilization strategies in MM patients who had only received VCD induction prior to autograft.
Methods
Retrospective review of PBSC mobilization strategies in patients from six apheresis centres from November 2012 to March 2015 after receiving VCD induction. Extended data were collected from a single centre to January 2016. Prior radiotherapy was not an exclusion criterion. Successful mobilization was defined as achieving physician-determined target PBSC yield, which in some older patients was ≥2x106/kg but in most patients was ≥4x106/kg to allow for two autografts (≥90% of both groups). Plerixafor was used in some centres as a rescue strategy if PB CD34 ≤10x106/L on the day of planned collection or PBSC yield was <1x106/kg after first apheresis. Univariate analysis was performed using chi-squared test for categorical data and Mann-Whitney-U test for continuous variables.
Results
Table 1 summarizes the results of 192 patients. Baseline characteristics and cumulative exposure to bortezomib and cyclophosphamide were similar in both groups. G-alone strategy consisted of G-CSF at 10μg/kg/day (n=120) or 20μg/kg /day (n=16), administered for a median of 5 days. G-cyclo comprised of intravenous cyclophosphamide (1g/m2 (n=1), 1.5g/m2 (n=14), 2g/m2 (n=25), 3g/m2 (n=4), 4g/m2 (n=12)) with either G-CSF 5-10μg/kg/day for a median of 4 days (n=35) or single-dose 6mg pegfilgrastim (n=21). Overall, the rates of successful mobilization and the proportion of patients achieving a total PBSC yield of ≥4x106/kg were comparable between G-alone and G-cyclo with no significant difference in the median number of aphereses to reach this target. However the G-cyclo group had a significantly higher median PBSC yield per apheresis and a higher proportion of patients attaining a PBSC yield of ≥4x106/kg with ≤2 apheresis without rescue plerixafor. Ten (18%) G-cyclo patients had unplanned hospitalization, of which 8 had febrile neutropenia. In the G-alone group, age ≤60 and G-CSF doses of 20μg/d were significantly associated with a higher median PBSC yield. In the G-cyclo group, higher cyclophosphamide doses for mobilization (3-4g/m2 vs 1-2g/m2) resulted in a significantly higher PBSC yield. Cumulative bortezomib doses, pre-mobilization platelet count and prior radiotherapy did not significantly impact on PBSC yield in either group.
Conclusion
Despite a significantly higher PBSC yield with G-cyclo mobilization, the G-alone strategy is a reasonable first approach to mobilizing stem cells in the majority of patients receiving VCD induction.
Session topic: E-poster
Keyword(s): Bortezomib, Myeloma, Stem cell mobilization
Type: Eposter Presentation
Background
Bortezomib, cyclophosphamide and dexamethasone (VCD) combination is often used as induction therapy in transplant eligible patients with multiple myeloma (MM). However, the optimal PBSC mobilization strategy in this context is not established.
Aims
To review the efficacy of G-CSF alone (G-alone) versus G-CSF and cyclophosphamide (G-cyclo) PBSC mobilization strategies in MM patients who had only received VCD induction prior to autograft.
Methods
Retrospective review of PBSC mobilization strategies in patients from six apheresis centres from November 2012 to March 2015 after receiving VCD induction. Extended data were collected from a single centre to January 2016. Prior radiotherapy was not an exclusion criterion. Successful mobilization was defined as achieving physician-determined target PBSC yield, which in some older patients was ≥2x106/kg but in most patients was ≥4x106/kg to allow for two autografts (≥90% of both groups). Plerixafor was used in some centres as a rescue strategy if PB CD34 ≤10x106/L on the day of planned collection or PBSC yield was <1x106/kg after first apheresis. Univariate analysis was performed using chi-squared test for categorical data and Mann-Whitney-U test for continuous variables.
Results
Table 1 summarizes the results of 192 patients. Baseline characteristics and cumulative exposure to bortezomib and cyclophosphamide were similar in both groups. G-alone strategy consisted of G-CSF at 10μg/kg/day (n=120) or 20μg/kg /day (n=16), administered for a median of 5 days. G-cyclo comprised of intravenous cyclophosphamide (1g/m2 (n=1), 1.5g/m2 (n=14), 2g/m2 (n=25), 3g/m2 (n=4), 4g/m2 (n=12)) with either G-CSF 5-10μg/kg/day for a median of 4 days (n=35) or single-dose 6mg pegfilgrastim (n=21). Overall, the rates of successful mobilization and the proportion of patients achieving a total PBSC yield of ≥4x106/kg were comparable between G-alone and G-cyclo with no significant difference in the median number of aphereses to reach this target. However the G-cyclo group had a significantly higher median PBSC yield per apheresis and a higher proportion of patients attaining a PBSC yield of ≥4x106/kg with ≤2 apheresis without rescue plerixafor. Ten (18%) G-cyclo patients had unplanned hospitalization, of which 8 had febrile neutropenia. In the G-alone group, age ≤60 and G-CSF doses of 20μg/d were significantly associated with a higher median PBSC yield. In the G-cyclo group, higher cyclophosphamide doses for mobilization (3-4g/m2 vs 1-2g/m2) resulted in a significantly higher PBSC yield. Cumulative bortezomib doses, pre-mobilization platelet count and prior radiotherapy did not significantly impact on PBSC yield in either group.
Conclusion
Despite a significantly higher PBSC yield with G-cyclo mobilization, the G-alone strategy is a reasonable first approach to mobilizing stem cells in the majority of patients receiving VCD induction.
Session topic: E-poster
Keyword(s): Bortezomib, Myeloma, Stem cell mobilization
{{ help_message }}
{{filter}}