
ANALYSIS OF T CELL SUBSETS IN G-CSF PRIMED BONE MARROW FOR ALLOGENEIC STEM CELL TRANSPLANTATION AND ITS ASSOCIATION WITH CHRONIC GVHD INCIDENCE
(Abstract release date: 05/19/16)
EHA Library. Leon Rodriguez E. 06/09/16; 132680; E1131

Dr. Eucario Leon Rodriguez
Contributions
Contributions
Abstract
Abstract: E1131
Type: Eposter Presentation
Background
There is a subset of T cells which modulate the immune system, maintain tolerance to self-antigens, and abrogate autoimmune disease, called regulatory T cells (Tregs). These cells generally suppress or downregulate induction and proliferation of effector T cells. Regulatory T cells come in many forms with the most well-understood being those that express CD4, CD25, and Foxp3 (CD4+CD25+ regulatory T cells). Mouse models of bone marrow transplantation as well as some clinical trials, have shown that the administration of Tregs in combination with the harvested bone marrow prevent and decrease graft-versus-host-disease (GVHD) and facilitate engraftment.At our institution the population transplanted with G-CSF primed bone marrow, has a lower incidence of chronic GVHD compared to those transplanted with peripheral blood and not primed bone marrow. Some microenvironment characteristics of this hematopoietic stem cells (HSC) source remain unknown, as well as the quantitative profile of different T cell subsets in patients who develop chronic GVHD and those who do not.
Aims
To analyze the characteristics of G-CSF primed bone marrow, identifying different T cell subsets, such as Th1, Th2, Th17, and Tregs. in 29 donor samples, between patients who developed chronic GVHD and those who did not.
Methods
A prospective analysis was performed in 29 G-CSF primed bone marrow samples from donors from 1999 to 2012. Mononuclear cells were defrosted, counted, and viability was assessed by trypan blue exclusion After a 24 hour resting time (RPMI), mononuclear cells were stimulated with PMA (50 ng/ml) for 48 hours and cells were harvested and stained for FACS analysis. Supernatants were collected and measured by Cytometric Bead Array. From each sample, one million mononuclear cells were permeabilized, fixed, and stained with CD4-FITC, IL17A-PE, IFN-γ APC, and IL-4 PECy7, and were analyzed by FACS. All samples were obtained in a BD LSR Fortessa cytometer and analyzed with the Flow-Jo software.Patients (recipients) demographic and clinical data were analyzed with support of the software SPSS v.21.
Results
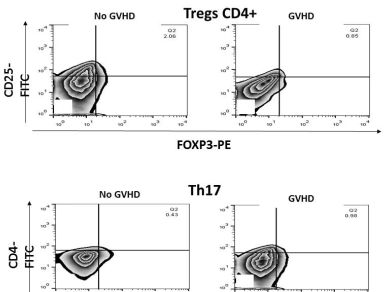
GVHD incidence was reported as following: Ten patients (34.5%) developed chronic GVHD (10% extensive, and 90% limited), and 16 patients did not present either.There was no difference in TH1 and TH2 numbers between both groups, but mononuclear cells from donors of patients who developed chronic GVHD had a higher percentage of Th17 cells (0.99% vs 0.44%, p<0.001), as well as decreased Tregs (0.91% vs 2.00%, p<0.001), compared to those who did not developed GVHD.It was not possible to relate T cell subsets with chronic GVHD severity since only one patient developed extensive disease.
Conclusion
With the usage of G-CSF primed bone marrow as a source of HSC, the incidence of chronic GVHD at our institution was 34.5%. Patients who develop chronic GVHD are characterized by a pro inflammatory response with a higher percentage of Th17 cells, as well as a decreased suppressive response characterized by reduced Tregs levels.The low incidence of chronic GVHD show that G-CSF primed bone marrow is an excellent source for allogeneic HSC transplantations, and would be useful to compare its lymphocyte subset profile and cytokines levels with other HSC sources.
Session topic: E-poster
Keyword(s): Bone Marrow, G-CSF, Graft-versus-host disease (GVHD), T cell
Type: Eposter Presentation
Background
There is a subset of T cells which modulate the immune system, maintain tolerance to self-antigens, and abrogate autoimmune disease, called regulatory T cells (Tregs). These cells generally suppress or downregulate induction and proliferation of effector T cells. Regulatory T cells come in many forms with the most well-understood being those that express CD4, CD25, and Foxp3 (CD4+CD25+ regulatory T cells). Mouse models of bone marrow transplantation as well as some clinical trials, have shown that the administration of Tregs in combination with the harvested bone marrow prevent and decrease graft-versus-host-disease (GVHD) and facilitate engraftment.At our institution the population transplanted with G-CSF primed bone marrow, has a lower incidence of chronic GVHD compared to those transplanted with peripheral blood and not primed bone marrow. Some microenvironment characteristics of this hematopoietic stem cells (HSC) source remain unknown, as well as the quantitative profile of different T cell subsets in patients who develop chronic GVHD and those who do not.
Aims
To analyze the characteristics of G-CSF primed bone marrow, identifying different T cell subsets, such as Th1, Th2, Th17, and Tregs. in 29 donor samples, between patients who developed chronic GVHD and those who did not.
Methods
A prospective analysis was performed in 29 G-CSF primed bone marrow samples from donors from 1999 to 2012. Mononuclear cells were defrosted, counted, and viability was assessed by trypan blue exclusion After a 24 hour resting time (RPMI), mononuclear cells were stimulated with PMA (50 ng/ml) for 48 hours and cells were harvested and stained for FACS analysis. Supernatants were collected and measured by Cytometric Bead Array. From each sample, one million mononuclear cells were permeabilized, fixed, and stained with CD4-FITC, IL17A-PE, IFN-γ APC, and IL-4 PECy7, and were analyzed by FACS. All samples were obtained in a BD LSR Fortessa cytometer and analyzed with the Flow-Jo software.Patients (recipients) demographic and clinical data were analyzed with support of the software SPSS v.21.
Results
GVHD incidence was reported as following: Ten patients (34.5%) developed chronic GVHD (10% extensive, and 90% limited), and 16 patients did not present either.There was no difference in TH1 and TH2 numbers between both groups, but mononuclear cells from donors of patients who developed chronic GVHD had a higher percentage of Th17 cells (0.99% vs 0.44%, p<0.001), as well as decreased Tregs (0.91% vs 2.00%, p<0.001), compared to those who did not developed GVHD.It was not possible to relate T cell subsets with chronic GVHD severity since only one patient developed extensive disease.
Conclusion
With the usage of G-CSF primed bone marrow as a source of HSC, the incidence of chronic GVHD at our institution was 34.5%. Patients who develop chronic GVHD are characterized by a pro inflammatory response with a higher percentage of Th17 cells, as well as a decreased suppressive response characterized by reduced Tregs levels.The low incidence of chronic GVHD show that G-CSF primed bone marrow is an excellent source for allogeneic HSC transplantations, and would be useful to compare its lymphocyte subset profile and cytokines levels with other HSC sources.
Session topic: E-poster
Keyword(s): Bone Marrow, G-CSF, Graft-versus-host disease (GVHD), T cell
Abstract: E1131
Type: Eposter Presentation
Background
There is a subset of T cells which modulate the immune system, maintain tolerance to self-antigens, and abrogate autoimmune disease, called regulatory T cells (Tregs). These cells generally suppress or downregulate induction and proliferation of effector T cells. Regulatory T cells come in many forms with the most well-understood being those that express CD4, CD25, and Foxp3 (CD4+CD25+ regulatory T cells). Mouse models of bone marrow transplantation as well as some clinical trials, have shown that the administration of Tregs in combination with the harvested bone marrow prevent and decrease graft-versus-host-disease (GVHD) and facilitate engraftment.At our institution the population transplanted with G-CSF primed bone marrow, has a lower incidence of chronic GVHD compared to those transplanted with peripheral blood and not primed bone marrow. Some microenvironment characteristics of this hematopoietic stem cells (HSC) source remain unknown, as well as the quantitative profile of different T cell subsets in patients who develop chronic GVHD and those who do not.
Aims
To analyze the characteristics of G-CSF primed bone marrow, identifying different T cell subsets, such as Th1, Th2, Th17, and Tregs. in 29 donor samples, between patients who developed chronic GVHD and those who did not.
Methods
A prospective analysis was performed in 29 G-CSF primed bone marrow samples from donors from 1999 to 2012. Mononuclear cells were defrosted, counted, and viability was assessed by trypan blue exclusion After a 24 hour resting time (RPMI), mononuclear cells were stimulated with PMA (50 ng/ml) for 48 hours and cells were harvested and stained for FACS analysis. Supernatants were collected and measured by Cytometric Bead Array. From each sample, one million mononuclear cells were permeabilized, fixed, and stained with CD4-FITC, IL17A-PE, IFN-γ APC, and IL-4 PECy7, and were analyzed by FACS. All samples were obtained in a BD LSR Fortessa cytometer and analyzed with the Flow-Jo software.Patients (recipients) demographic and clinical data were analyzed with support of the software SPSS v.21.
Results
GVHD incidence was reported as following: Ten patients (34.5%) developed chronic GVHD (10% extensive, and 90% limited), and 16 patients did not present either.There was no difference in TH1 and TH2 numbers between both groups, but mononuclear cells from donors of patients who developed chronic GVHD had a higher percentage of Th17 cells (0.99% vs 0.44%, p<0.001), as well as decreased Tregs (0.91% vs 2.00%, p<0.001), compared to those who did not developed GVHD.It was not possible to relate T cell subsets with chronic GVHD severity since only one patient developed extensive disease.
Conclusion
With the usage of G-CSF primed bone marrow as a source of HSC, the incidence of chronic GVHD at our institution was 34.5%. Patients who develop chronic GVHD are characterized by a pro inflammatory response with a higher percentage of Th17 cells, as well as a decreased suppressive response characterized by reduced Tregs levels.The low incidence of chronic GVHD show that G-CSF primed bone marrow is an excellent source for allogeneic HSC transplantations, and would be useful to compare its lymphocyte subset profile and cytokines levels with other HSC sources.
Session topic: E-poster
Keyword(s): Bone Marrow, G-CSF, Graft-versus-host disease (GVHD), T cell
Type: Eposter Presentation
Background
There is a subset of T cells which modulate the immune system, maintain tolerance to self-antigens, and abrogate autoimmune disease, called regulatory T cells (Tregs). These cells generally suppress or downregulate induction and proliferation of effector T cells. Regulatory T cells come in many forms with the most well-understood being those that express CD4, CD25, and Foxp3 (CD4+CD25+ regulatory T cells). Mouse models of bone marrow transplantation as well as some clinical trials, have shown that the administration of Tregs in combination with the harvested bone marrow prevent and decrease graft-versus-host-disease (GVHD) and facilitate engraftment.At our institution the population transplanted with G-CSF primed bone marrow, has a lower incidence of chronic GVHD compared to those transplanted with peripheral blood and not primed bone marrow. Some microenvironment characteristics of this hematopoietic stem cells (HSC) source remain unknown, as well as the quantitative profile of different T cell subsets in patients who develop chronic GVHD and those who do not.
Aims
To analyze the characteristics of G-CSF primed bone marrow, identifying different T cell subsets, such as Th1, Th2, Th17, and Tregs. in 29 donor samples, between patients who developed chronic GVHD and those who did not.
Methods
A prospective analysis was performed in 29 G-CSF primed bone marrow samples from donors from 1999 to 2012. Mononuclear cells were defrosted, counted, and viability was assessed by trypan blue exclusion After a 24 hour resting time (RPMI), mononuclear cells were stimulated with PMA (50 ng/ml) for 48 hours and cells were harvested and stained for FACS analysis. Supernatants were collected and measured by Cytometric Bead Array. From each sample, one million mononuclear cells were permeabilized, fixed, and stained with CD4-FITC, IL17A-PE, IFN-γ APC, and IL-4 PECy7, and were analyzed by FACS. All samples were obtained in a BD LSR Fortessa cytometer and analyzed with the Flow-Jo software.Patients (recipients) demographic and clinical data were analyzed with support of the software SPSS v.21.
Results
GVHD incidence was reported as following: Ten patients (34.5%) developed chronic GVHD (10% extensive, and 90% limited), and 16 patients did not present either.There was no difference in TH1 and TH2 numbers between both groups, but mononuclear cells from donors of patients who developed chronic GVHD had a higher percentage of Th17 cells (0.99% vs 0.44%, p<0.001), as well as decreased Tregs (0.91% vs 2.00%, p<0.001), compared to those who did not developed GVHD.It was not possible to relate T cell subsets with chronic GVHD severity since only one patient developed extensive disease.
Conclusion
With the usage of G-CSF primed bone marrow as a source of HSC, the incidence of chronic GVHD at our institution was 34.5%. Patients who develop chronic GVHD are characterized by a pro inflammatory response with a higher percentage of Th17 cells, as well as a decreased suppressive response characterized by reduced Tregs levels.The low incidence of chronic GVHD show that G-CSF primed bone marrow is an excellent source for allogeneic HSC transplantations, and would be useful to compare its lymphocyte subset profile and cytokines levels with other HSC sources.
Session topic: E-poster
Keyword(s): Bone Marrow, G-CSF, Graft-versus-host disease (GVHD), T cell
{{ help_message }}
{{filter}}