
SURVIVAL IN CHRONIC LYMPHOCYTIC LEUKEMIA: A POPULATION-BASED STUDY INCLUDING 13,034 PATIENTS DIAGNOSED IN 1982–2013 IN SWEDEN
(Abstract release date: 05/19/16)
EHA Library. Steingrímsson V. 06/09/16; 132600; E1051

Mr. Vilhjálmur Steingrímsson
Contributions
Contributions
Abstract
Abstract: E1051
Type: Eposter Presentation
Background
Chronic lymphocytic leukemia (CLL) is the most common leukemia in Western countries with a median age between 65-74 years at diagnosis. In clinical trials on CLL treatment, elderly patients with comorbidities have been heavily underrepresented and therefore population-based studies on survival are important to estimate effects of newer treatment on survival. Few observational studies on survival in CLL have been conducted and they have not been consistent in showing improved survival.
Aims
To evaluate the effect of the introduction of new drugs on survival in CLL patients, we conducted a population-based study in CLL patients diagnosed in Sweden from 1982 until 2013, with follow-up through 2014.
Methods
Information on CLL patients diagnosed between January 1, 1982 and December 31, 2013 was retrieved from the well-established Swedish Cancer Registry. The registry has been validated with regards to CLL and has a diagnostic accuracy of more than 90%. Relative survival ratios (RSR) and excess hazard ratios (EHR) were used for estimating the impact on patient survival.
Results
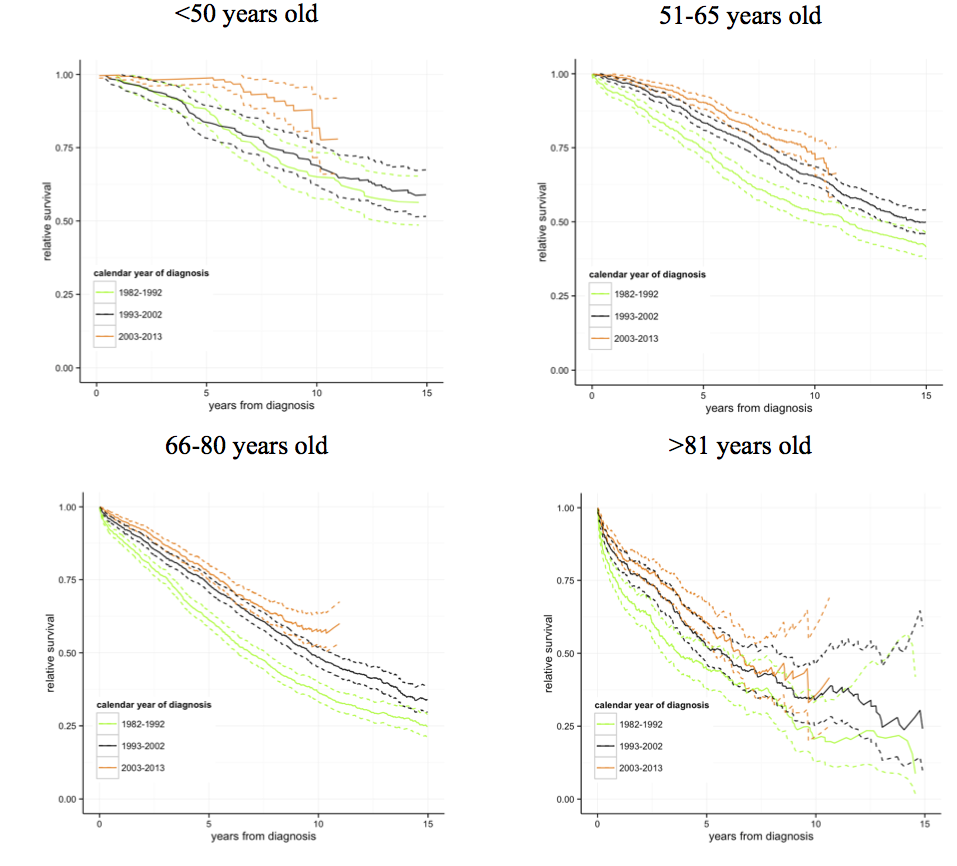
Between January 1, 1982 and December 31, 2013, a total of 13,034 CLL patients were reported to the Swedish Cancer Registry. Age was a significant predictor of survival reflected in reflected in EHRs of 1.48 (95% confidence interval (CI) 1.21-1.81), 2.69 (2.22-3.27) and 5.37 (4.33-6.66) for age groups 51-65, 66-80, and >81 years, respectively, compared to the reference interval of <50 years. Similar results were obtained when comparing 1-, 5- and 10-year survival between age groups. Males had a significantly increased excess risk of death compared to females (EHR=2.12, 95%, CI 1.93-2.34) and worse 1-, 5-, 10- and 15-year RSR. A significantly increased excess risk of death was observed in CLL patients diagnosed in the calendar period 1993-2002 compared to 2003-2013 (EHR=1.36; 95% CI 1.22-1.51). Furthermore, a significantly improved 5- and 10-year RSR was observed comparing CLL patients diagnosed 2003-2013 (5-year RSR 0.81, 95% CI 0.79-0.82 and 10-year RSR 0.61, 0.58-0.65) to 1993-2002 (0.75, 0.73-0.77 and 0.54, 0.51-0.56, respectively.When stratified by age groups, the excess risk of death was significantly higher in 1993-2002 compared to 2003-2013 in age groups <50, 51-65 and 66-80 years old, with EHR 2.87 (95% CI 1.52-5.42), 1.56 (1.26-1.93) and 1.25 (1.08-2.13), respectively. However, it was non-significant in patients 81 years and older (EHR=1.23, 95% CI 0.96-1.58). In age groups <50 and 51-65 years the 5-year survival was significantly better when calendar period 1993-2002 was compared to 2003-2013 (Figure). The 5-year RSR in age group <50 years old was 0.84 (95% CI 0.79-0.90) in 1993-2002 vs. 0.99 (95% CI 0.97-1.01) in 2003-2013 and in the age group 51-65 years the RSR was 0.84 (0.81-0.86) in 1993-2003 vs. 0.91 (0.89-0.93) in 2003-2013. The difference in 5-year RSR was non-significant in older age groups.
Conclusion
We have in this large population-based study, including more than 13,000 patients with CLL, shown improvement in survival of CLL patients in the last decade and the difference is most apparent in younger patients. Younger patients are in general healthier and less likely to have comorbidities. Based on our results we conclude that risk stratification is likely to benefit older patients for better selection of those patients that can receive intensive treatment. Furthermore, a more significant improvement in overall survival in elderly patients might be obtained with the introduction of a more targeted therapy with less side effects.
Session topic: E-poster
Keyword(s): Chronic lymphocytic leukemia, Population, Survival
Type: Eposter Presentation
Background
Chronic lymphocytic leukemia (CLL) is the most common leukemia in Western countries with a median age between 65-74 years at diagnosis. In clinical trials on CLL treatment, elderly patients with comorbidities have been heavily underrepresented and therefore population-based studies on survival are important to estimate effects of newer treatment on survival. Few observational studies on survival in CLL have been conducted and they have not been consistent in showing improved survival.
Aims
To evaluate the effect of the introduction of new drugs on survival in CLL patients, we conducted a population-based study in CLL patients diagnosed in Sweden from 1982 until 2013, with follow-up through 2014.
Methods
Information on CLL patients diagnosed between January 1, 1982 and December 31, 2013 was retrieved from the well-established Swedish Cancer Registry. The registry has been validated with regards to CLL and has a diagnostic accuracy of more than 90%. Relative survival ratios (RSR) and excess hazard ratios (EHR) were used for estimating the impact on patient survival.
Results
Between January 1, 1982 and December 31, 2013, a total of 13,034 CLL patients were reported to the Swedish Cancer Registry. Age was a significant predictor of survival reflected in reflected in EHRs of 1.48 (95% confidence interval (CI) 1.21-1.81), 2.69 (2.22-3.27) and 5.37 (4.33-6.66) for age groups 51-65, 66-80, and >81 years, respectively, compared to the reference interval of <50 years. Similar results were obtained when comparing 1-, 5- and 10-year survival between age groups. Males had a significantly increased excess risk of death compared to females (EHR=2.12, 95%, CI 1.93-2.34) and worse 1-, 5-, 10- and 15-year RSR. A significantly increased excess risk of death was observed in CLL patients diagnosed in the calendar period 1993-2002 compared to 2003-2013 (EHR=1.36; 95% CI 1.22-1.51). Furthermore, a significantly improved 5- and 10-year RSR was observed comparing CLL patients diagnosed 2003-2013 (5-year RSR 0.81, 95% CI 0.79-0.82 and 10-year RSR 0.61, 0.58-0.65) to 1993-2002 (0.75, 0.73-0.77 and 0.54, 0.51-0.56, respectively.When stratified by age groups, the excess risk of death was significantly higher in 1993-2002 compared to 2003-2013 in age groups <50, 51-65 and 66-80 years old, with EHR 2.87 (95% CI 1.52-5.42), 1.56 (1.26-1.93) and 1.25 (1.08-2.13), respectively. However, it was non-significant in patients 81 years and older (EHR=1.23, 95% CI 0.96-1.58). In age groups <50 and 51-65 years the 5-year survival was significantly better when calendar period 1993-2002 was compared to 2003-2013 (Figure). The 5-year RSR in age group <50 years old was 0.84 (95% CI 0.79-0.90) in 1993-2002 vs. 0.99 (95% CI 0.97-1.01) in 2003-2013 and in the age group 51-65 years the RSR was 0.84 (0.81-0.86) in 1993-2003 vs. 0.91 (0.89-0.93) in 2003-2013. The difference in 5-year RSR was non-significant in older age groups.
Conclusion
We have in this large population-based study, including more than 13,000 patients with CLL, shown improvement in survival of CLL patients in the last decade and the difference is most apparent in younger patients. Younger patients are in general healthier and less likely to have comorbidities. Based on our results we conclude that risk stratification is likely to benefit older patients for better selection of those patients that can receive intensive treatment. Furthermore, a more significant improvement in overall survival in elderly patients might be obtained with the introduction of a more targeted therapy with less side effects.
Session topic: E-poster
Keyword(s): Chronic lymphocytic leukemia, Population, Survival
Abstract: E1051
Type: Eposter Presentation
Background
Chronic lymphocytic leukemia (CLL) is the most common leukemia in Western countries with a median age between 65-74 years at diagnosis. In clinical trials on CLL treatment, elderly patients with comorbidities have been heavily underrepresented and therefore population-based studies on survival are important to estimate effects of newer treatment on survival. Few observational studies on survival in CLL have been conducted and they have not been consistent in showing improved survival.
Aims
To evaluate the effect of the introduction of new drugs on survival in CLL patients, we conducted a population-based study in CLL patients diagnosed in Sweden from 1982 until 2013, with follow-up through 2014.
Methods
Information on CLL patients diagnosed between January 1, 1982 and December 31, 2013 was retrieved from the well-established Swedish Cancer Registry. The registry has been validated with regards to CLL and has a diagnostic accuracy of more than 90%. Relative survival ratios (RSR) and excess hazard ratios (EHR) were used for estimating the impact on patient survival.
Results
Between January 1, 1982 and December 31, 2013, a total of 13,034 CLL patients were reported to the Swedish Cancer Registry. Age was a significant predictor of survival reflected in reflected in EHRs of 1.48 (95% confidence interval (CI) 1.21-1.81), 2.69 (2.22-3.27) and 5.37 (4.33-6.66) for age groups 51-65, 66-80, and >81 years, respectively, compared to the reference interval of <50 years. Similar results were obtained when comparing 1-, 5- and 10-year survival between age groups. Males had a significantly increased excess risk of death compared to females (EHR=2.12, 95%, CI 1.93-2.34) and worse 1-, 5-, 10- and 15-year RSR. A significantly increased excess risk of death was observed in CLL patients diagnosed in the calendar period 1993-2002 compared to 2003-2013 (EHR=1.36; 95% CI 1.22-1.51). Furthermore, a significantly improved 5- and 10-year RSR was observed comparing CLL patients diagnosed 2003-2013 (5-year RSR 0.81, 95% CI 0.79-0.82 and 10-year RSR 0.61, 0.58-0.65) to 1993-2002 (0.75, 0.73-0.77 and 0.54, 0.51-0.56, respectively.When stratified by age groups, the excess risk of death was significantly higher in 1993-2002 compared to 2003-2013 in age groups <50, 51-65 and 66-80 years old, with EHR 2.87 (95% CI 1.52-5.42), 1.56 (1.26-1.93) and 1.25 (1.08-2.13), respectively. However, it was non-significant in patients 81 years and older (EHR=1.23, 95% CI 0.96-1.58). In age groups <50 and 51-65 years the 5-year survival was significantly better when calendar period 1993-2002 was compared to 2003-2013 (Figure). The 5-year RSR in age group <50 years old was 0.84 (95% CI 0.79-0.90) in 1993-2002 vs. 0.99 (95% CI 0.97-1.01) in 2003-2013 and in the age group 51-65 years the RSR was 0.84 (0.81-0.86) in 1993-2003 vs. 0.91 (0.89-0.93) in 2003-2013. The difference in 5-year RSR was non-significant in older age groups.
Conclusion
We have in this large population-based study, including more than 13,000 patients with CLL, shown improvement in survival of CLL patients in the last decade and the difference is most apparent in younger patients. Younger patients are in general healthier and less likely to have comorbidities. Based on our results we conclude that risk stratification is likely to benefit older patients for better selection of those patients that can receive intensive treatment. Furthermore, a more significant improvement in overall survival in elderly patients might be obtained with the introduction of a more targeted therapy with less side effects.
Session topic: E-poster
Keyword(s): Chronic lymphocytic leukemia, Population, Survival
Type: Eposter Presentation
Background
Chronic lymphocytic leukemia (CLL) is the most common leukemia in Western countries with a median age between 65-74 years at diagnosis. In clinical trials on CLL treatment, elderly patients with comorbidities have been heavily underrepresented and therefore population-based studies on survival are important to estimate effects of newer treatment on survival. Few observational studies on survival in CLL have been conducted and they have not been consistent in showing improved survival.
Aims
To evaluate the effect of the introduction of new drugs on survival in CLL patients, we conducted a population-based study in CLL patients diagnosed in Sweden from 1982 until 2013, with follow-up through 2014.
Methods
Information on CLL patients diagnosed between January 1, 1982 and December 31, 2013 was retrieved from the well-established Swedish Cancer Registry. The registry has been validated with regards to CLL and has a diagnostic accuracy of more than 90%. Relative survival ratios (RSR) and excess hazard ratios (EHR) were used for estimating the impact on patient survival.
Results
Between January 1, 1982 and December 31, 2013, a total of 13,034 CLL patients were reported to the Swedish Cancer Registry. Age was a significant predictor of survival reflected in reflected in EHRs of 1.48 (95% confidence interval (CI) 1.21-1.81), 2.69 (2.22-3.27) and 5.37 (4.33-6.66) for age groups 51-65, 66-80, and >81 years, respectively, compared to the reference interval of <50 years. Similar results were obtained when comparing 1-, 5- and 10-year survival between age groups. Males had a significantly increased excess risk of death compared to females (EHR=2.12, 95%, CI 1.93-2.34) and worse 1-, 5-, 10- and 15-year RSR. A significantly increased excess risk of death was observed in CLL patients diagnosed in the calendar period 1993-2002 compared to 2003-2013 (EHR=1.36; 95% CI 1.22-1.51). Furthermore, a significantly improved 5- and 10-year RSR was observed comparing CLL patients diagnosed 2003-2013 (5-year RSR 0.81, 95% CI 0.79-0.82 and 10-year RSR 0.61, 0.58-0.65) to 1993-2002 (0.75, 0.73-0.77 and 0.54, 0.51-0.56, respectively.When stratified by age groups, the excess risk of death was significantly higher in 1993-2002 compared to 2003-2013 in age groups <50, 51-65 and 66-80 years old, with EHR 2.87 (95% CI 1.52-5.42), 1.56 (1.26-1.93) and 1.25 (1.08-2.13), respectively. However, it was non-significant in patients 81 years and older (EHR=1.23, 95% CI 0.96-1.58). In age groups <50 and 51-65 years the 5-year survival was significantly better when calendar period 1993-2002 was compared to 2003-2013 (Figure). The 5-year RSR in age group <50 years old was 0.84 (95% CI 0.79-0.90) in 1993-2002 vs. 0.99 (95% CI 0.97-1.01) in 2003-2013 and in the age group 51-65 years the RSR was 0.84 (0.81-0.86) in 1993-2003 vs. 0.91 (0.89-0.93) in 2003-2013. The difference in 5-year RSR was non-significant in older age groups.
Conclusion
We have in this large population-based study, including more than 13,000 patients with CLL, shown improvement in survival of CLL patients in the last decade and the difference is most apparent in younger patients. Younger patients are in general healthier and less likely to have comorbidities. Based on our results we conclude that risk stratification is likely to benefit older patients for better selection of those patients that can receive intensive treatment. Furthermore, a more significant improvement in overall survival in elderly patients might be obtained with the introduction of a more targeted therapy with less side effects.
Session topic: E-poster
Keyword(s): Chronic lymphocytic leukemia, Population, Survival
{{ help_message }}
{{filter}}