
IS THAT MALE GENDER AN ADVERSE RISK FACTOR ONLY IN YOUNG PATIENTS WITH DIFFUSE LARGE B-CELL LYMPHOMA ?
(Abstract release date: 05/19/16)
EHA Library. Faiza T. 06/09/16; 132536; E987

Dr. Talbi Faiza
Contributions
Contributions
Abstract
Abstract: E987
Type: Eposter Presentation
Background
The International Prognostic Index (IPI) is the most important clinical tool for determining prognosis in diffuse large B-cell lymphoma (DLBCL). It incorporates five adverse risk factors: age above 60 years; Ann Arbor stage III or IV; elevated serumnlactate dehydrogenase (S-LDH); Eastern Cooperative Oncology Group (ECOG) performance status of 2 or higher; and involvement of two or mor extranodal sites. GUSTAF HEDSTRÖM was published in Acta Oncologica (in April 2015), one of the largest population-based studies of DLBCL presented (7166 patients were included), he found male gender to be a significant adverse risk factor compared to fertile women, without msurvival differences between genders in the older sub-population. According Nurith H, the reduced rate of NHL among females may be explained by direct effects of estrogens on lymphoma cell proliferation or by its effect on anti-tumor immune response : the influence of sex hormones on lymphoid malignancies has been the subject of clinical and in vitro research. Epidemiological studies highlighting the association between sex hormones and NHL have provided some clues. Lee and colleagues reported that an increasing number of pregnancies and live births is associated with a decreasing trend in the risk of DLBCL.
Aims
The primary objective of this study was to analyze the impact of gender on age in patients with newly diagnosed DLBCL.This retrospective study included 95 patients with diffuse large B cell lymphoma who were treated the Medical Hematology Department, HCA during the time period from 2000 to 2015.
Methods
We conducted a retrospective cohort study of all DLBCL patients diagnosed between 2000 and 2015, to evaluate the impact of gender for survival from DLBCL. Survival curves n were estimated according to the Kaplan-Meier method and associated log rank, a Cox model was used to evaluate the prognostic impact of clinical risk factors (age < vs≥52 y, ECOG≤ VS>2, stage I-II vs III-IV, LDH normal vs high, extranodal sites, IPI (0-5), IPI-a (0-3).
Results
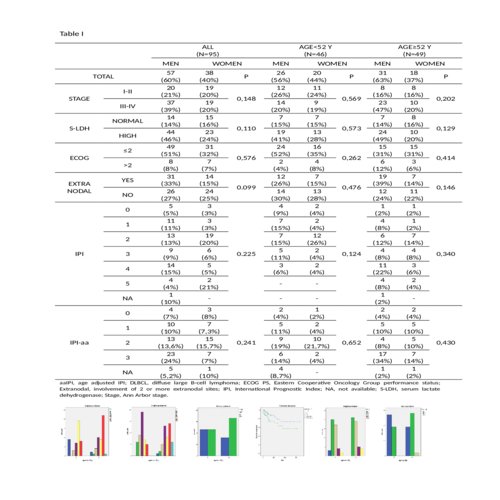
In total, 95 patients were included for analysis, clinical caracteristics of our patients are summarized in Table I. Data collected were: year of diagnosis, age, gender, Ann Arbor stage, ECOG performance status, extranodal sites, S-LDH, IPI, age adjusted IPI (aaIPI). When patients older (52 years or older), or younger than 52 years, were analysed separately, the same risk factors remained no significant.Sex was not found to be significantly correlated with adverse outcome in univariate analysis according to the Kaplan-Meier method and associated log rank tests: women have a comparable overall survival to that of men in the same age group (75% vs 88,5% ; P=0,332). nIn a relative survival multifactorial model adjusted for stage, ECOG performance status, serum lactate dehydrogenase and two or more extranodal sites, male gender was not found to be an adverse risk factor for patients younger than 52 years (RR 0.893, 95% CI 0.641 – 1.244). However, the impact of the above-mentioned prognostic factors was significantly correlated with age. In effect, using multiple regression Cox model, we found that Ann Arbor stage III and IV, as well as extranodal involvement of two or more sites, IPI are correlated to worse outcome, with 0.024 vs 0.087, 0.009 vs 0.844, 0.0001 vs 0.687 respectively, P (for age ≥ vs < 52 years), see Figure 1-6.
Conclusion
our study clearly demonstrates the impact of age on the survival of patients with LGDB, however gender does not appear to influence patient outcomes.
Session topic: E-poster
Keyword(s): B cell lymphoma, Malignant lymphoma
Type: Eposter Presentation
Background
The International Prognostic Index (IPI) is the most important clinical tool for determining prognosis in diffuse large B-cell lymphoma (DLBCL). It incorporates five adverse risk factors: age above 60 years; Ann Arbor stage III or IV; elevated serumnlactate dehydrogenase (S-LDH); Eastern Cooperative Oncology Group (ECOG) performance status of 2 or higher; and involvement of two or mor extranodal sites. GUSTAF HEDSTRÖM was published in Acta Oncologica (in April 2015), one of the largest population-based studies of DLBCL presented (7166 patients were included), he found male gender to be a significant adverse risk factor compared to fertile women, without msurvival differences between genders in the older sub-population. According Nurith H, the reduced rate of NHL among females may be explained by direct effects of estrogens on lymphoma cell proliferation or by its effect on anti-tumor immune response : the influence of sex hormones on lymphoid malignancies has been the subject of clinical and in vitro research. Epidemiological studies highlighting the association between sex hormones and NHL have provided some clues. Lee and colleagues reported that an increasing number of pregnancies and live births is associated with a decreasing trend in the risk of DLBCL.
Aims
The primary objective of this study was to analyze the impact of gender on age in patients with newly diagnosed DLBCL.This retrospective study included 95 patients with diffuse large B cell lymphoma who were treated the Medical Hematology Department, HCA during the time period from 2000 to 2015.
Methods
We conducted a retrospective cohort study of all DLBCL patients diagnosed between 2000 and 2015, to evaluate the impact of gender for survival from DLBCL. Survival curves n were estimated according to the Kaplan-Meier method and associated log rank, a Cox model was used to evaluate the prognostic impact of clinical risk factors (age < vs≥52 y, ECOG≤ VS>2, stage I-II vs III-IV, LDH normal vs high, extranodal sites, IPI (0-5), IPI-a (0-3).
Results
In total, 95 patients were included for analysis, clinical caracteristics of our patients are summarized in Table I. Data collected were: year of diagnosis, age, gender, Ann Arbor stage, ECOG performance status, extranodal sites, S-LDH, IPI, age adjusted IPI (aaIPI). When patients older (52 years or older), or younger than 52 years, were analysed separately, the same risk factors remained no significant.Sex was not found to be significantly correlated with adverse outcome in univariate analysis according to the Kaplan-Meier method and associated log rank tests: women have a comparable overall survival to that of men in the same age group (75% vs 88,5% ; P=0,332). nIn a relative survival multifactorial model adjusted for stage, ECOG performance status, serum lactate dehydrogenase and two or more extranodal sites, male gender was not found to be an adverse risk factor for patients younger than 52 years (RR 0.893, 95% CI 0.641 – 1.244). However, the impact of the above-mentioned prognostic factors was significantly correlated with age. In effect, using multiple regression Cox model, we found that Ann Arbor stage III and IV, as well as extranodal involvement of two or more sites, IPI are correlated to worse outcome, with 0.024 vs 0.087, 0.009 vs 0.844, 0.0001 vs 0.687 respectively, P (for age ≥ vs < 52 years), see Figure 1-6.
Conclusion
our study clearly demonstrates the impact of age on the survival of patients with LGDB, however gender does not appear to influence patient outcomes.
Session topic: E-poster
Keyword(s): B cell lymphoma, Malignant lymphoma
Abstract: E987
Type: Eposter Presentation
Background
The International Prognostic Index (IPI) is the most important clinical tool for determining prognosis in diffuse large B-cell lymphoma (DLBCL). It incorporates five adverse risk factors: age above 60 years; Ann Arbor stage III or IV; elevated serumnlactate dehydrogenase (S-LDH); Eastern Cooperative Oncology Group (ECOG) performance status of 2 or higher; and involvement of two or mor extranodal sites. GUSTAF HEDSTRÖM was published in Acta Oncologica (in April 2015), one of the largest population-based studies of DLBCL presented (7166 patients were included), he found male gender to be a significant adverse risk factor compared to fertile women, without msurvival differences between genders in the older sub-population. According Nurith H, the reduced rate of NHL among females may be explained by direct effects of estrogens on lymphoma cell proliferation or by its effect on anti-tumor immune response : the influence of sex hormones on lymphoid malignancies has been the subject of clinical and in vitro research. Epidemiological studies highlighting the association between sex hormones and NHL have provided some clues. Lee and colleagues reported that an increasing number of pregnancies and live births is associated with a decreasing trend in the risk of DLBCL.
Aims
The primary objective of this study was to analyze the impact of gender on age in patients with newly diagnosed DLBCL.This retrospective study included 95 patients with diffuse large B cell lymphoma who were treated the Medical Hematology Department, HCA during the time period from 2000 to 2015.
Methods
We conducted a retrospective cohort study of all DLBCL patients diagnosed between 2000 and 2015, to evaluate the impact of gender for survival from DLBCL. Survival curves n were estimated according to the Kaplan-Meier method and associated log rank, a Cox model was used to evaluate the prognostic impact of clinical risk factors (age < vs≥52 y, ECOG≤ VS>2, stage I-II vs III-IV, LDH normal vs high, extranodal sites, IPI (0-5), IPI-a (0-3).
Results
In total, 95 patients were included for analysis, clinical caracteristics of our patients are summarized in Table I. Data collected were: year of diagnosis, age, gender, Ann Arbor stage, ECOG performance status, extranodal sites, S-LDH, IPI, age adjusted IPI (aaIPI). When patients older (52 years or older), or younger than 52 years, were analysed separately, the same risk factors remained no significant.Sex was not found to be significantly correlated with adverse outcome in univariate analysis according to the Kaplan-Meier method and associated log rank tests: women have a comparable overall survival to that of men in the same age group (75% vs 88,5% ; P=0,332). nIn a relative survival multifactorial model adjusted for stage, ECOG performance status, serum lactate dehydrogenase and two or more extranodal sites, male gender was not found to be an adverse risk factor for patients younger than 52 years (RR 0.893, 95% CI 0.641 – 1.244). However, the impact of the above-mentioned prognostic factors was significantly correlated with age. In effect, using multiple regression Cox model, we found that Ann Arbor stage III and IV, as well as extranodal involvement of two or more sites, IPI are correlated to worse outcome, with 0.024 vs 0.087, 0.009 vs 0.844, 0.0001 vs 0.687 respectively, P (for age ≥ vs < 52 years), see Figure 1-6.
Conclusion
our study clearly demonstrates the impact of age on the survival of patients with LGDB, however gender does not appear to influence patient outcomes.
Session topic: E-poster
Keyword(s): B cell lymphoma, Malignant lymphoma
Type: Eposter Presentation
Background
The International Prognostic Index (IPI) is the most important clinical tool for determining prognosis in diffuse large B-cell lymphoma (DLBCL). It incorporates five adverse risk factors: age above 60 years; Ann Arbor stage III or IV; elevated serumnlactate dehydrogenase (S-LDH); Eastern Cooperative Oncology Group (ECOG) performance status of 2 or higher; and involvement of two or mor extranodal sites. GUSTAF HEDSTRÖM was published in Acta Oncologica (in April 2015), one of the largest population-based studies of DLBCL presented (7166 patients were included), he found male gender to be a significant adverse risk factor compared to fertile women, without msurvival differences between genders in the older sub-population. According Nurith H, the reduced rate of NHL among females may be explained by direct effects of estrogens on lymphoma cell proliferation or by its effect on anti-tumor immune response : the influence of sex hormones on lymphoid malignancies has been the subject of clinical and in vitro research. Epidemiological studies highlighting the association between sex hormones and NHL have provided some clues. Lee and colleagues reported that an increasing number of pregnancies and live births is associated with a decreasing trend in the risk of DLBCL.
Aims
The primary objective of this study was to analyze the impact of gender on age in patients with newly diagnosed DLBCL.This retrospective study included 95 patients with diffuse large B cell lymphoma who were treated the Medical Hematology Department, HCA during the time period from 2000 to 2015.
Methods
We conducted a retrospective cohort study of all DLBCL patients diagnosed between 2000 and 2015, to evaluate the impact of gender for survival from DLBCL. Survival curves n were estimated according to the Kaplan-Meier method and associated log rank, a Cox model was used to evaluate the prognostic impact of clinical risk factors (age < vs≥52 y, ECOG≤ VS>2, stage I-II vs III-IV, LDH normal vs high, extranodal sites, IPI (0-5), IPI-a (0-3).
Results
In total, 95 patients were included for analysis, clinical caracteristics of our patients are summarized in Table I. Data collected were: year of diagnosis, age, gender, Ann Arbor stage, ECOG performance status, extranodal sites, S-LDH, IPI, age adjusted IPI (aaIPI). When patients older (52 years or older), or younger than 52 years, were analysed separately, the same risk factors remained no significant.Sex was not found to be significantly correlated with adverse outcome in univariate analysis according to the Kaplan-Meier method and associated log rank tests: women have a comparable overall survival to that of men in the same age group (75% vs 88,5% ; P=0,332). nIn a relative survival multifactorial model adjusted for stage, ECOG performance status, serum lactate dehydrogenase and two or more extranodal sites, male gender was not found to be an adverse risk factor for patients younger than 52 years (RR 0.893, 95% CI 0.641 – 1.244). However, the impact of the above-mentioned prognostic factors was significantly correlated with age. In effect, using multiple regression Cox model, we found that Ann Arbor stage III and IV, as well as extranodal involvement of two or more sites, IPI are correlated to worse outcome, with 0.024 vs 0.087, 0.009 vs 0.844, 0.0001 vs 0.687 respectively, P (for age ≥ vs < 52 years), see Figure 1-6.
Conclusion
our study clearly demonstrates the impact of age on the survival of patients with LGDB, however gender does not appear to influence patient outcomes.
Session topic: E-poster
Keyword(s): B cell lymphoma, Malignant lymphoma
{{ help_message }}
{{filter}}