
ELDERLY AGE IS NOT EXCLUSION FACTOR FOR INTENSIVE THERAPY BY SCHEME R-DA-EPOCH/R-HMA FOR PATIENTS WITH UNTREATED HIGH-GRADE DIFFUSE LARGE B-CELL LYMPHOMA.
(Abstract release date: 05/19/16)
EHA Library. Aleshina (Gavrilina) O. 06/09/16; 132529; E980

Dr. Olga Aleshina (Gavrilina)
Contributions
Contributions
Abstract
Abstract: E980
Type: Eposter Presentation
Background
Median of age for patients with diffuse large B-cell lymphoma (DLBCL) is 60. Approximately 50% of DLBCL are defined as high-grade by IPI and these forms are characterized by aggressive course and poor response to standard chemotherapy (CT). High-dose methotrexate courses, as example Hyper-CVAD/HMA or mNHL-BFM-90 protocols are applied for patients with high risk DLBCL. But for elder patients this approach usually is not employed due to the extreme toxicity. Addition of R-HMA to R-DA-EPOCH favourably changes the outcome in patients with untreated high-grade diffuse large B-cell lymphoma [ASH 2015 # 2708].
Aims
To evaluate the efficacy and toxicity of R-DA-EPOCH/R-HMA protocol in patients with untreated high-grade diffuse large B-cell lymphoma depending on age.
Methods
35 untreated DLBCL patients from 4 centers were enrolled in a prospective study between August 2013 - Jan 2016; stage II-IV; ECOG 0-3; median age 55 years (27-76); age ≥60y/<60y 50%/50%; M/F 60%/40%; IPI: 63% high-intermediate and 37% high risk; 20% with bone marrow involvement. All patients underwent 4-8 courses (2-4 cycles) of chemotherapy: R-DA-EPOCH (standard dose and scheme), R-HMA (R 375 mg/m2 d1, MTX 1000 mg/m2 24 hours d 2, AraC 3000 mg/m2 q 12 hrs d 3-4). For patients older than 60 year dose of R-HMA was reduced (R 375 mg/m2 d1, MTX 500 mg/m2 24 hours d 2, AraC 1000 mg/m2 q 12 hrs d 3-4) and R-EPOCH were applied without dose adjusted. In 4 cases of DLBCL with bone marrow involvement BEAM conditioning and autologous stem cell transplantation were applied.
Results
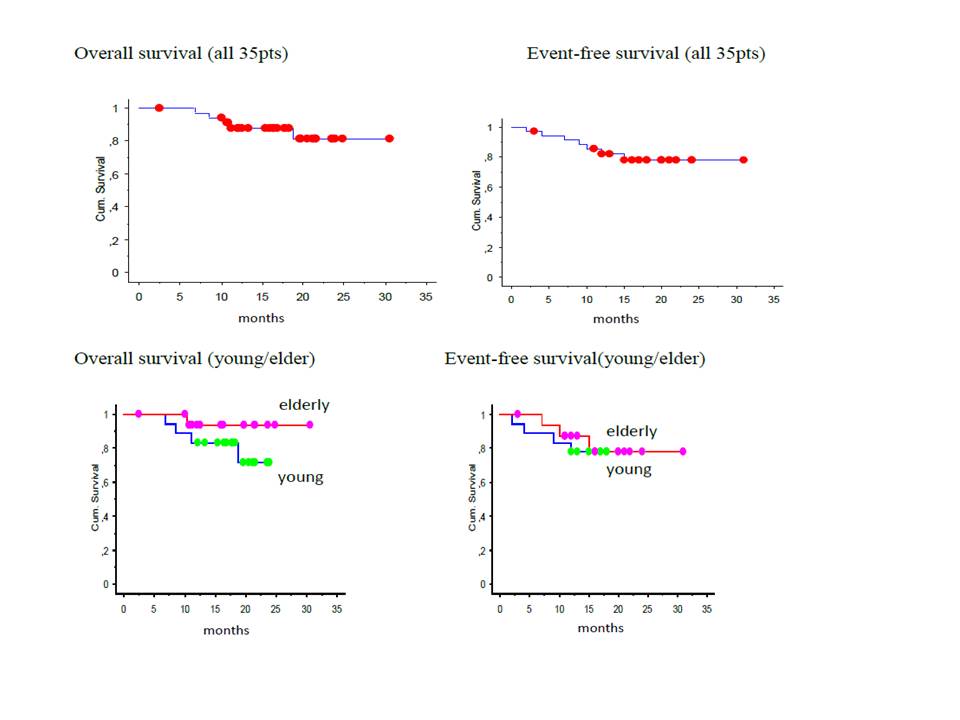
The median follow-up is 16 months (3-31). There was no mortality associated with toxicity. The main non-hematological toxicities of R-HMA were infections (mucositis, pneumonia, sepsis, enteropathy) grades 1-2 and 3-4 in 90% and 10%, respectively. Hematological toxicity grade 4 for less than 4 days we observed only after courses R-HMA. Complete remission (CR) was achieved in 31 (88,6%) patients. In group of young patients we observed 2 progressions of the disease after first cycle of chemotherapy, 2 cases with partial remission after 2-3 cycles and following progression of disease. There are three failures in patients older than 60 years: two relapses (after 5 and 13 month CR) and one death after 7 month CR by reasons not related with DLBCL.With a median follow 16 months overall and event-free survival of 35 patients constituted 81,6% and 78,2%, respectively. There is no difference in elderly and young groups: OS was 93,3% vs 71,4% (p=0,2), EFS was 77,8% in both. So the combination of R-DA-EPOCH/R-HMA may be considered as optimal intensive approach in elder patients.
Conclusion
The R-DA-EPOCH/R-HMA protocol demonstrated acceptable toxicity and high efficacy in patients with high-grade DLBCL. This protocol has shown optimistic results in the elderly patients and it could be recommended for further investigation in that group.
Session topic: E-poster
Keyword(s): Chemotherapy, Diffuse large B cell lymphoma, Elderly
Type: Eposter Presentation
Background
Median of age for patients with diffuse large B-cell lymphoma (DLBCL) is 60. Approximately 50% of DLBCL are defined as high-grade by IPI and these forms are characterized by aggressive course and poor response to standard chemotherapy (CT). High-dose methotrexate courses, as example Hyper-CVAD/HMA or mNHL-BFM-90 protocols are applied for patients with high risk DLBCL. But for elder patients this approach usually is not employed due to the extreme toxicity. Addition of R-HMA to R-DA-EPOCH favourably changes the outcome in patients with untreated high-grade diffuse large B-cell lymphoma [ASH 2015 # 2708].
Aims
To evaluate the efficacy and toxicity of R-DA-EPOCH/R-HMA protocol in patients with untreated high-grade diffuse large B-cell lymphoma depending on age.
Methods
35 untreated DLBCL patients from 4 centers were enrolled in a prospective study between August 2013 - Jan 2016; stage II-IV; ECOG 0-3; median age 55 years (27-76); age ≥60y/<60y 50%/50%; M/F 60%/40%; IPI: 63% high-intermediate and 37% high risk; 20% with bone marrow involvement. All patients underwent 4-8 courses (2-4 cycles) of chemotherapy: R-DA-EPOCH (standard dose and scheme), R-HMA (R 375 mg/m2 d1, MTX 1000 mg/m2 24 hours d 2, AraC 3000 mg/m2 q 12 hrs d 3-4). For patients older than 60 year dose of R-HMA was reduced (R 375 mg/m2 d1, MTX 500 mg/m2 24 hours d 2, AraC 1000 mg/m2 q 12 hrs d 3-4) and R-EPOCH were applied without dose adjusted. In 4 cases of DLBCL with bone marrow involvement BEAM conditioning and autologous stem cell transplantation were applied.
Results
The median follow-up is 16 months (3-31). There was no mortality associated with toxicity. The main non-hematological toxicities of R-HMA were infections (mucositis, pneumonia, sepsis, enteropathy) grades 1-2 and 3-4 in 90% and 10%, respectively. Hematological toxicity grade 4 for less than 4 days we observed only after courses R-HMA. Complete remission (CR) was achieved in 31 (88,6%) patients. In group of young patients we observed 2 progressions of the disease after first cycle of chemotherapy, 2 cases with partial remission after 2-3 cycles and following progression of disease. There are three failures in patients older than 60 years: two relapses (after 5 and 13 month CR) and one death after 7 month CR by reasons not related with DLBCL.With a median follow 16 months overall and event-free survival of 35 patients constituted 81,6% and 78,2%, respectively. There is no difference in elderly and young groups: OS was 93,3% vs 71,4% (p=0,2), EFS was 77,8% in both. So the combination of R-DA-EPOCH/R-HMA may be considered as optimal intensive approach in elder patients.
Conclusion
The R-DA-EPOCH/R-HMA protocol demonstrated acceptable toxicity and high efficacy in patients with high-grade DLBCL. This protocol has shown optimistic results in the elderly patients and it could be recommended for further investigation in that group.
Session topic: E-poster
Keyword(s): Chemotherapy, Diffuse large B cell lymphoma, Elderly
Abstract: E980
Type: Eposter Presentation
Background
Median of age for patients with diffuse large B-cell lymphoma (DLBCL) is 60. Approximately 50% of DLBCL are defined as high-grade by IPI and these forms are characterized by aggressive course and poor response to standard chemotherapy (CT). High-dose methotrexate courses, as example Hyper-CVAD/HMA or mNHL-BFM-90 protocols are applied for patients with high risk DLBCL. But for elder patients this approach usually is not employed due to the extreme toxicity. Addition of R-HMA to R-DA-EPOCH favourably changes the outcome in patients with untreated high-grade diffuse large B-cell lymphoma [ASH 2015 # 2708].
Aims
To evaluate the efficacy and toxicity of R-DA-EPOCH/R-HMA protocol in patients with untreated high-grade diffuse large B-cell lymphoma depending on age.
Methods
35 untreated DLBCL patients from 4 centers were enrolled in a prospective study between August 2013 - Jan 2016; stage II-IV; ECOG 0-3; median age 55 years (27-76); age ≥60y/<60y 50%/50%; M/F 60%/40%; IPI: 63% high-intermediate and 37% high risk; 20% with bone marrow involvement. All patients underwent 4-8 courses (2-4 cycles) of chemotherapy: R-DA-EPOCH (standard dose and scheme), R-HMA (R 375 mg/m2 d1, MTX 1000 mg/m2 24 hours d 2, AraC 3000 mg/m2 q 12 hrs d 3-4). For patients older than 60 year dose of R-HMA was reduced (R 375 mg/m2 d1, MTX 500 mg/m2 24 hours d 2, AraC 1000 mg/m2 q 12 hrs d 3-4) and R-EPOCH were applied without dose adjusted. In 4 cases of DLBCL with bone marrow involvement BEAM conditioning and autologous stem cell transplantation were applied.
Results
The median follow-up is 16 months (3-31). There was no mortality associated with toxicity. The main non-hematological toxicities of R-HMA were infections (mucositis, pneumonia, sepsis, enteropathy) grades 1-2 and 3-4 in 90% and 10%, respectively. Hematological toxicity grade 4 for less than 4 days we observed only after courses R-HMA. Complete remission (CR) was achieved in 31 (88,6%) patients. In group of young patients we observed 2 progressions of the disease after first cycle of chemotherapy, 2 cases with partial remission after 2-3 cycles and following progression of disease. There are three failures in patients older than 60 years: two relapses (after 5 and 13 month CR) and one death after 7 month CR by reasons not related with DLBCL.With a median follow 16 months overall and event-free survival of 35 patients constituted 81,6% and 78,2%, respectively. There is no difference in elderly and young groups: OS was 93,3% vs 71,4% (p=0,2), EFS was 77,8% in both. So the combination of R-DA-EPOCH/R-HMA may be considered as optimal intensive approach in elder patients.
Conclusion
The R-DA-EPOCH/R-HMA protocol demonstrated acceptable toxicity and high efficacy in patients with high-grade DLBCL. This protocol has shown optimistic results in the elderly patients and it could be recommended for further investigation in that group.
Session topic: E-poster
Keyword(s): Chemotherapy, Diffuse large B cell lymphoma, Elderly
Type: Eposter Presentation
Background
Median of age for patients with diffuse large B-cell lymphoma (DLBCL) is 60. Approximately 50% of DLBCL are defined as high-grade by IPI and these forms are characterized by aggressive course and poor response to standard chemotherapy (CT). High-dose methotrexate courses, as example Hyper-CVAD/HMA or mNHL-BFM-90 protocols are applied for patients with high risk DLBCL. But for elder patients this approach usually is not employed due to the extreme toxicity. Addition of R-HMA to R-DA-EPOCH favourably changes the outcome in patients with untreated high-grade diffuse large B-cell lymphoma [ASH 2015 # 2708].
Aims
To evaluate the efficacy and toxicity of R-DA-EPOCH/R-HMA protocol in patients with untreated high-grade diffuse large B-cell lymphoma depending on age.
Methods
35 untreated DLBCL patients from 4 centers were enrolled in a prospective study between August 2013 - Jan 2016; stage II-IV; ECOG 0-3; median age 55 years (27-76); age ≥60y/<60y 50%/50%; M/F 60%/40%; IPI: 63% high-intermediate and 37% high risk; 20% with bone marrow involvement. All patients underwent 4-8 courses (2-4 cycles) of chemotherapy: R-DA-EPOCH (standard dose and scheme), R-HMA (R 375 mg/m2 d1, MTX 1000 mg/m2 24 hours d 2, AraC 3000 mg/m2 q 12 hrs d 3-4). For patients older than 60 year dose of R-HMA was reduced (R 375 mg/m2 d1, MTX 500 mg/m2 24 hours d 2, AraC 1000 mg/m2 q 12 hrs d 3-4) and R-EPOCH were applied without dose adjusted. In 4 cases of DLBCL with bone marrow involvement BEAM conditioning and autologous stem cell transplantation were applied.
Results
The median follow-up is 16 months (3-31). There was no mortality associated with toxicity. The main non-hematological toxicities of R-HMA were infections (mucositis, pneumonia, sepsis, enteropathy) grades 1-2 and 3-4 in 90% and 10%, respectively. Hematological toxicity grade 4 for less than 4 days we observed only after courses R-HMA. Complete remission (CR) was achieved in 31 (88,6%) patients. In group of young patients we observed 2 progressions of the disease after first cycle of chemotherapy, 2 cases with partial remission after 2-3 cycles and following progression of disease. There are three failures in patients older than 60 years: two relapses (after 5 and 13 month CR) and one death after 7 month CR by reasons not related with DLBCL.With a median follow 16 months overall and event-free survival of 35 patients constituted 81,6% and 78,2%, respectively. There is no difference in elderly and young groups: OS was 93,3% vs 71,4% (p=0,2), EFS was 77,8% in both. So the combination of R-DA-EPOCH/R-HMA may be considered as optimal intensive approach in elder patients.
Conclusion
The R-DA-EPOCH/R-HMA protocol demonstrated acceptable toxicity and high efficacy in patients with high-grade DLBCL. This protocol has shown optimistic results in the elderly patients and it could be recommended for further investigation in that group.
Session topic: E-poster
Keyword(s): Chemotherapy, Diffuse large B cell lymphoma, Elderly
{{ help_message }}
{{filter}}