
TREATMENT OF INITIAL CENTRAL NERVOUS SYSTEM INVOLVEMENT IN SYSTEMIC AGGRESSIVE LYMPHOMA WITH HIGH DOSE METHOTREXATE AND R-CHOP
(Abstract release date: 05/19/16)
EHA Library. Nijland M. 06/09/16; 132520; E971

Mr. Marcel Nijland
Contributions
Contributions
Abstract
Abstract: E971
Type: Eposter Presentation
Background
Central nervous system (CNS) involvement in systemic aggressive B-cell non Hodgkin lymphomas (B-NHL) at initial diagnosis is uncommon. Two recent studies suggest a beneficial effect of intensive chemotherapy followed by autologous stem cell transplantation (ASCT) for these patients, but since ASCT was only offered to patients in complete remission optimal treatment remains unclear.
Aims
We investigated the outcome of patients with concomitant systemic and CNS B-NHL (sCNS B-NHL) at diagnosis treated with high dose methotrexate (HD-MTX) and R-CHOP, but no ASCT.
Methods
We performed a retrospective cohort study of patients with sCNS B-NHL at diagnosis identified from the electronical databases of 2 referral centers in the Netherlands. Patients had histological proven aggressive B-NHL and stage 4 disease according to Ann Arbor classification with concomitant parynchymal CNS involvement. Patients were treated according to one of two regimens: either 6 alternating cycles of HD-MTX and R-CHOP, or four cycles of HD-MTX followed by 6 cycles of R-CHOP. In the latter MTX was part of the MBVP regimen which also includes teniposide (VP16) and carmustine (BCNU). Primary endpoints were progression free survival (PFS) and overall survival (OS).
Results
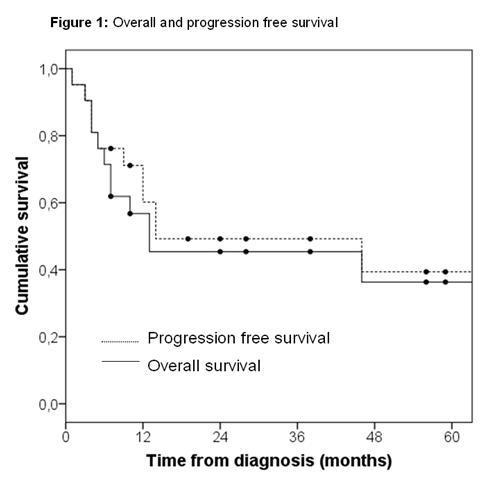
From 2001-2015 21 patients with sCNS B-NHL were identified. Median follow-up was 28 months. Characteristics at diagnosis: median age 54 years (range 19-71); WHO performance ≥ 2: 33%; IPI-score 0-1: 9%, 2-3: 66%, 4-5: 25%. Histological B-NHL types: diffuse large B-cell lymphoma: 66%; iatrogenic immunodeficiency B-NHL: 14%; transformed marginal zone lymphoma: 10%; intravascular B-NHL: 10%. Systemic organ involvement: testicular: 44% of patients at risk; breast: 17% of patients at risk; bone: 38%; kidney: 19%. Concomitant spinal fluid localization occured in 43% of patients. Fifteen out of 21 patients completed therapy as planned. The median number of MTX cycles at a dose of 3 g/m2 was 4 (range 1-8). Sixty-two percent of patients also received intrathecal MTX. The median number of R-CHOP cycles was 6 (range 0-8). Whole brain radiotherapy was given to 33% of patients in partial remission. Besides the additional VP16 and BCNU in patients treated with MBVP, there was no difference between the two regimens. 3-year PFS and OS for the entire cohort were 45% (95%CI 34-56%) and 49% (95%CI 38-60%) respectively. The treatment related mortality (TRM) was 24% (5/21). No significant difference in OS was found between the two regimens (HR OS 1.25, 95%CI 0.38-4.2 p 0.72). The 3 patients with IPI-score 0-1 were alive at the last control, whereas all 4 patients with IPI-score 4-5 died within 2 years after diagnosis. There were 6 relapses (28%): 2 systemic, 2 in CNS, and 2 both systemic and in CNS.
Conclusion
In this second largest cohort described to date, the outcome of patients with sCNS B-NHL treated with HD-MTX and R-CHOP was comparable to that of more intensive regimens. Prospective studies are needed to define the optimal treatment for these patients.
Session topic: E-poster
Keyword(s): B cell lymphoma, CHOP, CNS lymphoma, Methotrexate
Type: Eposter Presentation
Background
Central nervous system (CNS) involvement in systemic aggressive B-cell non Hodgkin lymphomas (B-NHL) at initial diagnosis is uncommon. Two recent studies suggest a beneficial effect of intensive chemotherapy followed by autologous stem cell transplantation (ASCT) for these patients, but since ASCT was only offered to patients in complete remission optimal treatment remains unclear.
Aims
We investigated the outcome of patients with concomitant systemic and CNS B-NHL (sCNS B-NHL) at diagnosis treated with high dose methotrexate (HD-MTX) and R-CHOP, but no ASCT.
Methods
We performed a retrospective cohort study of patients with sCNS B-NHL at diagnosis identified from the electronical databases of 2 referral centers in the Netherlands. Patients had histological proven aggressive B-NHL and stage 4 disease according to Ann Arbor classification with concomitant parynchymal CNS involvement. Patients were treated according to one of two regimens: either 6 alternating cycles of HD-MTX and R-CHOP, or four cycles of HD-MTX followed by 6 cycles of R-CHOP. In the latter MTX was part of the MBVP regimen which also includes teniposide (VP16) and carmustine (BCNU). Primary endpoints were progression free survival (PFS) and overall survival (OS).
Results
From 2001-2015 21 patients with sCNS B-NHL were identified. Median follow-up was 28 months. Characteristics at diagnosis: median age 54 years (range 19-71); WHO performance ≥ 2: 33%; IPI-score 0-1: 9%, 2-3: 66%, 4-5: 25%. Histological B-NHL types: diffuse large B-cell lymphoma: 66%; iatrogenic immunodeficiency B-NHL: 14%; transformed marginal zone lymphoma: 10%; intravascular B-NHL: 10%. Systemic organ involvement: testicular: 44% of patients at risk; breast: 17% of patients at risk; bone: 38%; kidney: 19%. Concomitant spinal fluid localization occured in 43% of patients. Fifteen out of 21 patients completed therapy as planned. The median number of MTX cycles at a dose of 3 g/m2 was 4 (range 1-8). Sixty-two percent of patients also received intrathecal MTX. The median number of R-CHOP cycles was 6 (range 0-8). Whole brain radiotherapy was given to 33% of patients in partial remission. Besides the additional VP16 and BCNU in patients treated with MBVP, there was no difference between the two regimens. 3-year PFS and OS for the entire cohort were 45% (95%CI 34-56%) and 49% (95%CI 38-60%) respectively. The treatment related mortality (TRM) was 24% (5/21). No significant difference in OS was found between the two regimens (HR OS 1.25, 95%CI 0.38-4.2 p 0.72). The 3 patients with IPI-score 0-1 were alive at the last control, whereas all 4 patients with IPI-score 4-5 died within 2 years after diagnosis. There were 6 relapses (28%): 2 systemic, 2 in CNS, and 2 both systemic and in CNS.
Conclusion
In this second largest cohort described to date, the outcome of patients with sCNS B-NHL treated with HD-MTX and R-CHOP was comparable to that of more intensive regimens. Prospective studies are needed to define the optimal treatment for these patients.
Session topic: E-poster
Keyword(s): B cell lymphoma, CHOP, CNS lymphoma, Methotrexate
Abstract: E971
Type: Eposter Presentation
Background
Central nervous system (CNS) involvement in systemic aggressive B-cell non Hodgkin lymphomas (B-NHL) at initial diagnosis is uncommon. Two recent studies suggest a beneficial effect of intensive chemotherapy followed by autologous stem cell transplantation (ASCT) for these patients, but since ASCT was only offered to patients in complete remission optimal treatment remains unclear.
Aims
We investigated the outcome of patients with concomitant systemic and CNS B-NHL (sCNS B-NHL) at diagnosis treated with high dose methotrexate (HD-MTX) and R-CHOP, but no ASCT.
Methods
We performed a retrospective cohort study of patients with sCNS B-NHL at diagnosis identified from the electronical databases of 2 referral centers in the Netherlands. Patients had histological proven aggressive B-NHL and stage 4 disease according to Ann Arbor classification with concomitant parynchymal CNS involvement. Patients were treated according to one of two regimens: either 6 alternating cycles of HD-MTX and R-CHOP, or four cycles of HD-MTX followed by 6 cycles of R-CHOP. In the latter MTX was part of the MBVP regimen which also includes teniposide (VP16) and carmustine (BCNU). Primary endpoints were progression free survival (PFS) and overall survival (OS).
Results
From 2001-2015 21 patients with sCNS B-NHL were identified. Median follow-up was 28 months. Characteristics at diagnosis: median age 54 years (range 19-71); WHO performance ≥ 2: 33%; IPI-score 0-1: 9%, 2-3: 66%, 4-5: 25%. Histological B-NHL types: diffuse large B-cell lymphoma: 66%; iatrogenic immunodeficiency B-NHL: 14%; transformed marginal zone lymphoma: 10%; intravascular B-NHL: 10%. Systemic organ involvement: testicular: 44% of patients at risk; breast: 17% of patients at risk; bone: 38%; kidney: 19%. Concomitant spinal fluid localization occured in 43% of patients. Fifteen out of 21 patients completed therapy as planned. The median number of MTX cycles at a dose of 3 g/m2 was 4 (range 1-8). Sixty-two percent of patients also received intrathecal MTX. The median number of R-CHOP cycles was 6 (range 0-8). Whole brain radiotherapy was given to 33% of patients in partial remission. Besides the additional VP16 and BCNU in patients treated with MBVP, there was no difference between the two regimens. 3-year PFS and OS for the entire cohort were 45% (95%CI 34-56%) and 49% (95%CI 38-60%) respectively. The treatment related mortality (TRM) was 24% (5/21). No significant difference in OS was found between the two regimens (HR OS 1.25, 95%CI 0.38-4.2 p 0.72). The 3 patients with IPI-score 0-1 were alive at the last control, whereas all 4 patients with IPI-score 4-5 died within 2 years after diagnosis. There were 6 relapses (28%): 2 systemic, 2 in CNS, and 2 both systemic and in CNS.
Conclusion
In this second largest cohort described to date, the outcome of patients with sCNS B-NHL treated with HD-MTX and R-CHOP was comparable to that of more intensive regimens. Prospective studies are needed to define the optimal treatment for these patients.
Session topic: E-poster
Keyword(s): B cell lymphoma, CHOP, CNS lymphoma, Methotrexate
Type: Eposter Presentation
Background
Central nervous system (CNS) involvement in systemic aggressive B-cell non Hodgkin lymphomas (B-NHL) at initial diagnosis is uncommon. Two recent studies suggest a beneficial effect of intensive chemotherapy followed by autologous stem cell transplantation (ASCT) for these patients, but since ASCT was only offered to patients in complete remission optimal treatment remains unclear.
Aims
We investigated the outcome of patients with concomitant systemic and CNS B-NHL (sCNS B-NHL) at diagnosis treated with high dose methotrexate (HD-MTX) and R-CHOP, but no ASCT.
Methods
We performed a retrospective cohort study of patients with sCNS B-NHL at diagnosis identified from the electronical databases of 2 referral centers in the Netherlands. Patients had histological proven aggressive B-NHL and stage 4 disease according to Ann Arbor classification with concomitant parynchymal CNS involvement. Patients were treated according to one of two regimens: either 6 alternating cycles of HD-MTX and R-CHOP, or four cycles of HD-MTX followed by 6 cycles of R-CHOP. In the latter MTX was part of the MBVP regimen which also includes teniposide (VP16) and carmustine (BCNU). Primary endpoints were progression free survival (PFS) and overall survival (OS).
Results
From 2001-2015 21 patients with sCNS B-NHL were identified. Median follow-up was 28 months. Characteristics at diagnosis: median age 54 years (range 19-71); WHO performance ≥ 2: 33%; IPI-score 0-1: 9%, 2-3: 66%, 4-5: 25%. Histological B-NHL types: diffuse large B-cell lymphoma: 66%; iatrogenic immunodeficiency B-NHL: 14%; transformed marginal zone lymphoma: 10%; intravascular B-NHL: 10%. Systemic organ involvement: testicular: 44% of patients at risk; breast: 17% of patients at risk; bone: 38%; kidney: 19%. Concomitant spinal fluid localization occured in 43% of patients. Fifteen out of 21 patients completed therapy as planned. The median number of MTX cycles at a dose of 3 g/m2 was 4 (range 1-8). Sixty-two percent of patients also received intrathecal MTX. The median number of R-CHOP cycles was 6 (range 0-8). Whole brain radiotherapy was given to 33% of patients in partial remission. Besides the additional VP16 and BCNU in patients treated with MBVP, there was no difference between the two regimens. 3-year PFS and OS for the entire cohort were 45% (95%CI 34-56%) and 49% (95%CI 38-60%) respectively. The treatment related mortality (TRM) was 24% (5/21). No significant difference in OS was found between the two regimens (HR OS 1.25, 95%CI 0.38-4.2 p 0.72). The 3 patients with IPI-score 0-1 were alive at the last control, whereas all 4 patients with IPI-score 4-5 died within 2 years after diagnosis. There were 6 relapses (28%): 2 systemic, 2 in CNS, and 2 both systemic and in CNS.
Conclusion
In this second largest cohort described to date, the outcome of patients with sCNS B-NHL treated with HD-MTX and R-CHOP was comparable to that of more intensive regimens. Prospective studies are needed to define the optimal treatment for these patients.
Session topic: E-poster
Keyword(s): B cell lymphoma, CHOP, CNS lymphoma, Methotrexate
{{ help_message }}
{{filter}}