
GENOTYPIC AND PHENOTYPIC CLONAL EVOLUTION IN RELAPSED FAVORABLE-ACUTE MYELOID LEUKEMIA PATIENTS
(Abstract release date: 05/19/16)
EHA Library. Martinez Losada C. 06/09/16; 132488; E939

Ms. Carmen Martinez Losada
Contributions
Contributions
Abstract
Abstract: E939
Type: Eposter Presentation
Background
Despite high rates of cure with standard chemotherapy in patients with favourable-risk acute myeloid leukemia (AML) according to European Leukemia Net (ELN) classification, some patients will eventually relapse. It is currently unclear whether leukaemia relapse is due to intrinsic chemo resistance or to clonal evolution with acquisition of new driver mutations and clonal selection
Aims
Characterization of phenotypic and genotypic features at relapse compared to diagnosis in patients with molecular/cytogenetic favourable-risk AML presenting relapse after achieving complete remission (CR).
Methods
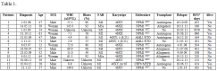
Retrospective study of 13 molecular/cytogenetic low risk AML patients (Non-M3) (CBF 3 NPM1 10) according to ELN classification criteria from Tor Vergata Hospital (Rome) and Reina Sofia Hospital (Córdoba). They were treated with intensive chemotherapy achieving CR and relapsed after a median of 12.2 months (4.4-255.9) (Table 1). NRAS, KRAS, DNMT3A, IDH1, IDH2 and TP53 genes were analyzed in marrow samples obtained at relapse by Sanger Sequencing using ABI 3130® Genetic Analyzer (Applied Biosystems Inc., Foster City, CA). When a mutation was found, the diagnosis sample for this mutation was screened using Sanger Sequencing also. A complete phenotypic profile was carried out using multiparametric flow cytometry with 3-laser FACSCanto II in both diagnosis and relapse samples. Additionally, all mutations were tested at diagnosis in 7 patients with favourable-risk AML achieving continuous CR (non-relapsing patients)
Results
In non-relapsing patients, only a case with IDH1 mutation (R132H) was found. When analyzing relapse-diagnosis paired samples in 13 AML patients, three patterns of clonal evolution were found:Group A (8 patients): Genotypic (G) and phenotypic (P) persistence of the main clone. Two patients presented a mutation in DNMT3A gene: R882H mutation and c.2705_2706delTC (p.F902fs) mutation (not described so far) respectively. Both mutations were found in diagnosis and relapse samples and phenotypic profile remained unchanged.Group B (2 patients): Phenotypic profile evolution but no changes in genotype. One patient harboured a mutation in DNMT3A gene (R882H) in both diagnosis and relapse samples. Many importants phenotypic changes were observed: In diagnosis sample, CD65+, CD19-, CD15+, CD117+, DR+, CD56LOW, CD7-, CD13+, CD2+, CD11b+, CD14-, CD38+, CD34+, CD33+ were expressed in the main leukemic clone. In the relapse sample, CD15, DR, CD56, CD2 and CD11b not expressed. Group C: 3 patients presented phenotypic and genotypic clonal evolution. The mutations were detected in relapse but not in diagnosis samples: i) D876Y mutation in DNMT3A gene (not described so far), accompanied with phenotypic profile changes with acquisition of CD34 and CD117 and loss of CD15. ii) R140Q mutation in IDH2 gene and G105 mutation in IDH1 gene with a phenotypic evolution with acquisition of CD34 and loss of a suclone CD56 +. iii) G105 in IDH1 gene with a phenotypic evolution with increased of CD33 and acquisition of CD15. These mutations were studied by NGS in the diagnosis samples. IDH mutations were present in both patients, while DNMT3A gene remained wild type.
Conclusion
i). Driver mutations are found more frequently in patients with favourable-risk AML who relapse compared to those with sustained CR . ii). 3 patterns of relapse were detected: A). No P changes / G (N = 8); B). P Changes / No G (N = 2). C). P changes / G (N = 3). These results highlight the importance of clonal evolution at relapse in favourable-risk AML patients.
Session topic: E-poster
Type: Eposter Presentation
Background
Despite high rates of cure with standard chemotherapy in patients with favourable-risk acute myeloid leukemia (AML) according to European Leukemia Net (ELN) classification, some patients will eventually relapse. It is currently unclear whether leukaemia relapse is due to intrinsic chemo resistance or to clonal evolution with acquisition of new driver mutations and clonal selection
Aims
Characterization of phenotypic and genotypic features at relapse compared to diagnosis in patients with molecular/cytogenetic favourable-risk AML presenting relapse after achieving complete remission (CR).
Methods
Retrospective study of 13 molecular/cytogenetic low risk AML patients (Non-M3) (CBF 3 NPM1 10) according to ELN classification criteria from Tor Vergata Hospital (Rome) and Reina Sofia Hospital (Córdoba). They were treated with intensive chemotherapy achieving CR and relapsed after a median of 12.2 months (4.4-255.9) (Table 1). NRAS, KRAS, DNMT3A, IDH1, IDH2 and TP53 genes were analyzed in marrow samples obtained at relapse by Sanger Sequencing using ABI 3130® Genetic Analyzer (Applied Biosystems Inc., Foster City, CA). When a mutation was found, the diagnosis sample for this mutation was screened using Sanger Sequencing also. A complete phenotypic profile was carried out using multiparametric flow cytometry with 3-laser FACSCanto II in both diagnosis and relapse samples. Additionally, all mutations were tested at diagnosis in 7 patients with favourable-risk AML achieving continuous CR (non-relapsing patients)
Results
In non-relapsing patients, only a case with IDH1 mutation (R132H) was found. When analyzing relapse-diagnosis paired samples in 13 AML patients, three patterns of clonal evolution were found:Group A (8 patients): Genotypic (G) and phenotypic (P) persistence of the main clone. Two patients presented a mutation in DNMT3A gene: R882H mutation and c.2705_2706delTC (p.F902fs) mutation (not described so far) respectively. Both mutations were found in diagnosis and relapse samples and phenotypic profile remained unchanged.Group B (2 patients): Phenotypic profile evolution but no changes in genotype. One patient harboured a mutation in DNMT3A gene (R882H) in both diagnosis and relapse samples. Many importants phenotypic changes were observed: In diagnosis sample, CD65+, CD19-, CD15+, CD117+, DR+, CD56LOW, CD7-, CD13+, CD2+, CD11b+, CD14-, CD38+, CD34+, CD33+ were expressed in the main leukemic clone. In the relapse sample, CD15, DR, CD56, CD2 and CD11b not expressed. Group C: 3 patients presented phenotypic and genotypic clonal evolution. The mutations were detected in relapse but not in diagnosis samples: i) D876Y mutation in DNMT3A gene (not described so far), accompanied with phenotypic profile changes with acquisition of CD34 and CD117 and loss of CD15. ii) R140Q mutation in IDH2 gene and G105 mutation in IDH1 gene with a phenotypic evolution with acquisition of CD34 and loss of a suclone CD56 +. iii) G105 in IDH1 gene with a phenotypic evolution with increased of CD33 and acquisition of CD15. These mutations were studied by NGS in the diagnosis samples. IDH mutations were present in both patients, while DNMT3A gene remained wild type.
Conclusion
i). Driver mutations are found more frequently in patients with favourable-risk AML who relapse compared to those with sustained CR . ii). 3 patterns of relapse were detected: A). No P changes / G (N = 8); B). P Changes / No G (N = 2). C). P changes / G (N = 3). These results highlight the importance of clonal evolution at relapse in favourable-risk AML patients.
Session topic: E-poster
Abstract: E939
Type: Eposter Presentation
Background
Despite high rates of cure with standard chemotherapy in patients with favourable-risk acute myeloid leukemia (AML) according to European Leukemia Net (ELN) classification, some patients will eventually relapse. It is currently unclear whether leukaemia relapse is due to intrinsic chemo resistance or to clonal evolution with acquisition of new driver mutations and clonal selection
Aims
Characterization of phenotypic and genotypic features at relapse compared to diagnosis in patients with molecular/cytogenetic favourable-risk AML presenting relapse after achieving complete remission (CR).
Methods
Retrospective study of 13 molecular/cytogenetic low risk AML patients (Non-M3) (CBF 3 NPM1 10) according to ELN classification criteria from Tor Vergata Hospital (Rome) and Reina Sofia Hospital (Córdoba). They were treated with intensive chemotherapy achieving CR and relapsed after a median of 12.2 months (4.4-255.9) (Table 1). NRAS, KRAS, DNMT3A, IDH1, IDH2 and TP53 genes were analyzed in marrow samples obtained at relapse by Sanger Sequencing using ABI 3130® Genetic Analyzer (Applied Biosystems Inc., Foster City, CA). When a mutation was found, the diagnosis sample for this mutation was screened using Sanger Sequencing also. A complete phenotypic profile was carried out using multiparametric flow cytometry with 3-laser FACSCanto II in both diagnosis and relapse samples. Additionally, all mutations were tested at diagnosis in 7 patients with favourable-risk AML achieving continuous CR (non-relapsing patients)
Results
In non-relapsing patients, only a case with IDH1 mutation (R132H) was found. When analyzing relapse-diagnosis paired samples in 13 AML patients, three patterns of clonal evolution were found:Group A (8 patients): Genotypic (G) and phenotypic (P) persistence of the main clone. Two patients presented a mutation in DNMT3A gene: R882H mutation and c.2705_2706delTC (p.F902fs) mutation (not described so far) respectively. Both mutations were found in diagnosis and relapse samples and phenotypic profile remained unchanged.Group B (2 patients): Phenotypic profile evolution but no changes in genotype. One patient harboured a mutation in DNMT3A gene (R882H) in both diagnosis and relapse samples. Many importants phenotypic changes were observed: In diagnosis sample, CD65+, CD19-, CD15+, CD117+, DR+, CD56LOW, CD7-, CD13+, CD2+, CD11b+, CD14-, CD38+, CD34+, CD33+ were expressed in the main leukemic clone. In the relapse sample, CD15, DR, CD56, CD2 and CD11b not expressed. Group C: 3 patients presented phenotypic and genotypic clonal evolution. The mutations were detected in relapse but not in diagnosis samples: i) D876Y mutation in DNMT3A gene (not described so far), accompanied with phenotypic profile changes with acquisition of CD34 and CD117 and loss of CD15. ii) R140Q mutation in IDH2 gene and G105 mutation in IDH1 gene with a phenotypic evolution with acquisition of CD34 and loss of a suclone CD56 +. iii) G105 in IDH1 gene with a phenotypic evolution with increased of CD33 and acquisition of CD15. These mutations were studied by NGS in the diagnosis samples. IDH mutations were present in both patients, while DNMT3A gene remained wild type.
Conclusion
i). Driver mutations are found more frequently in patients with favourable-risk AML who relapse compared to those with sustained CR . ii). 3 patterns of relapse were detected: A). No P changes / G (N = 8); B). P Changes / No G (N = 2). C). P changes / G (N = 3). These results highlight the importance of clonal evolution at relapse in favourable-risk AML patients.
Session topic: E-poster
Type: Eposter Presentation
Background
Despite high rates of cure with standard chemotherapy in patients with favourable-risk acute myeloid leukemia (AML) according to European Leukemia Net (ELN) classification, some patients will eventually relapse. It is currently unclear whether leukaemia relapse is due to intrinsic chemo resistance or to clonal evolution with acquisition of new driver mutations and clonal selection
Aims
Characterization of phenotypic and genotypic features at relapse compared to diagnosis in patients with molecular/cytogenetic favourable-risk AML presenting relapse after achieving complete remission (CR).
Methods
Retrospective study of 13 molecular/cytogenetic low risk AML patients (Non-M3) (CBF 3 NPM1 10) according to ELN classification criteria from Tor Vergata Hospital (Rome) and Reina Sofia Hospital (Córdoba). They were treated with intensive chemotherapy achieving CR and relapsed after a median of 12.2 months (4.4-255.9) (Table 1). NRAS, KRAS, DNMT3A, IDH1, IDH2 and TP53 genes were analyzed in marrow samples obtained at relapse by Sanger Sequencing using ABI 3130® Genetic Analyzer (Applied Biosystems Inc., Foster City, CA). When a mutation was found, the diagnosis sample for this mutation was screened using Sanger Sequencing also. A complete phenotypic profile was carried out using multiparametric flow cytometry with 3-laser FACSCanto II in both diagnosis and relapse samples. Additionally, all mutations were tested at diagnosis in 7 patients with favourable-risk AML achieving continuous CR (non-relapsing patients)
Results
In non-relapsing patients, only a case with IDH1 mutation (R132H) was found. When analyzing relapse-diagnosis paired samples in 13 AML patients, three patterns of clonal evolution were found:Group A (8 patients): Genotypic (G) and phenotypic (P) persistence of the main clone. Two patients presented a mutation in DNMT3A gene: R882H mutation and c.2705_2706delTC (p.F902fs) mutation (not described so far) respectively. Both mutations were found in diagnosis and relapse samples and phenotypic profile remained unchanged.Group B (2 patients): Phenotypic profile evolution but no changes in genotype. One patient harboured a mutation in DNMT3A gene (R882H) in both diagnosis and relapse samples. Many importants phenotypic changes were observed: In diagnosis sample, CD65+, CD19-, CD15+, CD117+, DR+, CD56LOW, CD7-, CD13+, CD2+, CD11b+, CD14-, CD38+, CD34+, CD33+ were expressed in the main leukemic clone. In the relapse sample, CD15, DR, CD56, CD2 and CD11b not expressed. Group C: 3 patients presented phenotypic and genotypic clonal evolution. The mutations were detected in relapse but not in diagnosis samples: i) D876Y mutation in DNMT3A gene (not described so far), accompanied with phenotypic profile changes with acquisition of CD34 and CD117 and loss of CD15. ii) R140Q mutation in IDH2 gene and G105 mutation in IDH1 gene with a phenotypic evolution with acquisition of CD34 and loss of a suclone CD56 +. iii) G105 in IDH1 gene with a phenotypic evolution with increased of CD33 and acquisition of CD15. These mutations were studied by NGS in the diagnosis samples. IDH mutations were present in both patients, while DNMT3A gene remained wild type.
Conclusion
i). Driver mutations are found more frequently in patients with favourable-risk AML who relapse compared to those with sustained CR . ii). 3 patterns of relapse were detected: A). No P changes / G (N = 8); B). P Changes / No G (N = 2). C). P changes / G (N = 3). These results highlight the importance of clonal evolution at relapse in favourable-risk AML patients.
Session topic: E-poster
{{ help_message }}
{{filter}}