
INTENSIVE VS. SEMI-INTENSIVE CHEMOTHERAPY IN OLDER ADULTS (55-65 YR) WITH PHILADELPHIA CHROMOSOME-NEGATIVE ACUTE LYMPHOBLASTIC LEUKEMIA.
(Abstract release date: 05/19/16)
EHA Library. Ribera J. 06/09/16; 132409; E860
Disclosure(s): Supported in part with the grants PI10/01417 from Fondo de Investigaciones Sanitarias and RD12/0036/0029 from RTICC, Instituto Carlos III and 2014SGR225(GRE), Generalitat de Catalunya, Spain, and a grant from “La Caixa” Foundation.

Josep-Maria Ribera
Contributions
Contributions
Abstract
Abstract: E860
Type: Eposter Presentation
Background
Treatment of older adults (55-65 yr.) with ALL is difficult to standardize. The election between intensive vs. semi-intensive therapy is frequently based on physician and/or patient preferences. Specific analyses of outcomes according to the intensity of the therapy in this age group are scarce.
Aims
To analyze and compare the baseline characteristics, the results of treatment and the outcomes of older adults (55-65yr.) with Ph-negative ALL included in intensive high-risk (HR) protocols (ALL03 and ALL11, J Clin Oncol 2014; 32:1595-604, Blood 2015; 126: 1333) vs. semi-intensive protocols (ALLOLD07, Leuk Res 2016; 41: 12-20) from the Spanish PETHEMA Group.
Methods
The main clinical and hematologic data, as well as the response to therapy and outcome of older adults (55-65 yr.) with Ph-negative ALL treated intensively or semi-intensively according to the PETHEMA protocols were analyzed and compared. Intensive protocols (ALL03 and ALL11) included intensive induction and consolidation therapy followed by allogeneic HSCT according to MRD clearance. Semi-intensive protocol (ALLOLD07) includes non-intensive induction chemotherapy with non-genotoxic drugs, followed by semi-intensive consolidation and standard maintenance therapy (EWALL backbone); allogeneic HSCT with RIC regimen was allowed in fit patients in CR1 according to physician’s criteria.
Results
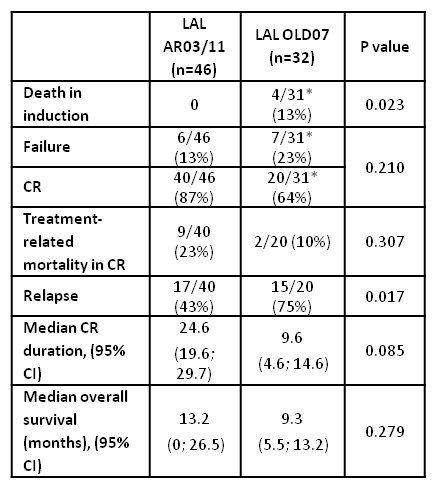
From 2003 to 2015, 46 patients were treated intensively vs. 32 treated semi-intensively. Except for age (intensive: 58[55-65] yr. vs. semi-intenive: 61 [56-65], p=0.01), the main clinical and hematological characteristics at baseline were comparable in the two groups. Death in induction and relapse rate were higher in the semi-intensive group, with a trend for a lower CR duration in this group. However, the OS probability was not significantly different in the two groups (Table 1). The rate of HSCT realization in CR1 was low in both groups (8% vs. 5%).
Conclusion
This study confirms the poor prognosis of older adults (55-65 yr.) with Ph-negative ALL, regardless of the intensity of the therapy. The low rate of HSCT in CR1 in this age group and a high rate of death in consolidation in patients treated intensively are of note. The trend for a significantly better CR duration in patients treated intensively did not translate into improved OS. Better therapies are needed in this age group of Ph-negative ALL patients. Supported in part with the grants PI10/01417 from Fondo de Investigaciones Sanitarias and RD12/0036/0029 from RTICC, Instituto Carlos III and 2014SGR225(GRE), Generalitat de Catalunya, Spain, and a grant from “La Caixa” Foundation.
Session topic: E-poster
Keyword(s): Acute lymphoblastic leukemia, Old, Prognosis, Treatment
Type: Eposter Presentation
Background
Treatment of older adults (55-65 yr.) with ALL is difficult to standardize. The election between intensive vs. semi-intensive therapy is frequently based on physician and/or patient preferences. Specific analyses of outcomes according to the intensity of the therapy in this age group are scarce.
Aims
To analyze and compare the baseline characteristics, the results of treatment and the outcomes of older adults (55-65yr.) with Ph-negative ALL included in intensive high-risk (HR) protocols (ALL03 and ALL11, J Clin Oncol 2014; 32:1595-604, Blood 2015; 126: 1333) vs. semi-intensive protocols (ALLOLD07, Leuk Res 2016; 41: 12-20) from the Spanish PETHEMA Group.
Methods
The main clinical and hematologic data, as well as the response to therapy and outcome of older adults (55-65 yr.) with Ph-negative ALL treated intensively or semi-intensively according to the PETHEMA protocols were analyzed and compared. Intensive protocols (ALL03 and ALL11) included intensive induction and consolidation therapy followed by allogeneic HSCT according to MRD clearance. Semi-intensive protocol (ALLOLD07) includes non-intensive induction chemotherapy with non-genotoxic drugs, followed by semi-intensive consolidation and standard maintenance therapy (EWALL backbone); allogeneic HSCT with RIC regimen was allowed in fit patients in CR1 according to physician’s criteria.
Results
From 2003 to 2015, 46 patients were treated intensively vs. 32 treated semi-intensively. Except for age (intensive: 58[55-65] yr. vs. semi-intenive: 61 [56-65], p=0.01), the main clinical and hematological characteristics at baseline were comparable in the two groups. Death in induction and relapse rate were higher in the semi-intensive group, with a trend for a lower CR duration in this group. However, the OS probability was not significantly different in the two groups (Table 1). The rate of HSCT realization in CR1 was low in both groups (8% vs. 5%).
Conclusion
This study confirms the poor prognosis of older adults (55-65 yr.) with Ph-negative ALL, regardless of the intensity of the therapy. The low rate of HSCT in CR1 in this age group and a high rate of death in consolidation in patients treated intensively are of note. The trend for a significantly better CR duration in patients treated intensively did not translate into improved OS. Better therapies are needed in this age group of Ph-negative ALL patients. Supported in part with the grants PI10/01417 from Fondo de Investigaciones Sanitarias and RD12/0036/0029 from RTICC, Instituto Carlos III and 2014SGR225(GRE), Generalitat de Catalunya, Spain, and a grant from “La Caixa” Foundation.
Session topic: E-poster
Keyword(s): Acute lymphoblastic leukemia, Old, Prognosis, Treatment
Abstract: E860
Type: Eposter Presentation
Background
Treatment of older adults (55-65 yr.) with ALL is difficult to standardize. The election between intensive vs. semi-intensive therapy is frequently based on physician and/or patient preferences. Specific analyses of outcomes according to the intensity of the therapy in this age group are scarce.
Aims
To analyze and compare the baseline characteristics, the results of treatment and the outcomes of older adults (55-65yr.) with Ph-negative ALL included in intensive high-risk (HR) protocols (ALL03 and ALL11, J Clin Oncol 2014; 32:1595-604, Blood 2015; 126: 1333) vs. semi-intensive protocols (ALLOLD07, Leuk Res 2016; 41: 12-20) from the Spanish PETHEMA Group.
Methods
The main clinical and hematologic data, as well as the response to therapy and outcome of older adults (55-65 yr.) with Ph-negative ALL treated intensively or semi-intensively according to the PETHEMA protocols were analyzed and compared. Intensive protocols (ALL03 and ALL11) included intensive induction and consolidation therapy followed by allogeneic HSCT according to MRD clearance. Semi-intensive protocol (ALLOLD07) includes non-intensive induction chemotherapy with non-genotoxic drugs, followed by semi-intensive consolidation and standard maintenance therapy (EWALL backbone); allogeneic HSCT with RIC regimen was allowed in fit patients in CR1 according to physician’s criteria.
Results
From 2003 to 2015, 46 patients were treated intensively vs. 32 treated semi-intensively. Except for age (intensive: 58[55-65] yr. vs. semi-intenive: 61 [56-65], p=0.01), the main clinical and hematological characteristics at baseline were comparable in the two groups. Death in induction and relapse rate were higher in the semi-intensive group, with a trend for a lower CR duration in this group. However, the OS probability was not significantly different in the two groups (Table 1). The rate of HSCT realization in CR1 was low in both groups (8% vs. 5%).
Conclusion
This study confirms the poor prognosis of older adults (55-65 yr.) with Ph-negative ALL, regardless of the intensity of the therapy. The low rate of HSCT in CR1 in this age group and a high rate of death in consolidation in patients treated intensively are of note. The trend for a significantly better CR duration in patients treated intensively did not translate into improved OS. Better therapies are needed in this age group of Ph-negative ALL patients. Supported in part with the grants PI10/01417 from Fondo de Investigaciones Sanitarias and RD12/0036/0029 from RTICC, Instituto Carlos III and 2014SGR225(GRE), Generalitat de Catalunya, Spain, and a grant from “La Caixa” Foundation.
Session topic: E-poster
Keyword(s): Acute lymphoblastic leukemia, Old, Prognosis, Treatment
Type: Eposter Presentation
Background
Treatment of older adults (55-65 yr.) with ALL is difficult to standardize. The election between intensive vs. semi-intensive therapy is frequently based on physician and/or patient preferences. Specific analyses of outcomes according to the intensity of the therapy in this age group are scarce.
Aims
To analyze and compare the baseline characteristics, the results of treatment and the outcomes of older adults (55-65yr.) with Ph-negative ALL included in intensive high-risk (HR) protocols (ALL03 and ALL11, J Clin Oncol 2014; 32:1595-604, Blood 2015; 126: 1333) vs. semi-intensive protocols (ALLOLD07, Leuk Res 2016; 41: 12-20) from the Spanish PETHEMA Group.
Methods
The main clinical and hematologic data, as well as the response to therapy and outcome of older adults (55-65 yr.) with Ph-negative ALL treated intensively or semi-intensively according to the PETHEMA protocols were analyzed and compared. Intensive protocols (ALL03 and ALL11) included intensive induction and consolidation therapy followed by allogeneic HSCT according to MRD clearance. Semi-intensive protocol (ALLOLD07) includes non-intensive induction chemotherapy with non-genotoxic drugs, followed by semi-intensive consolidation and standard maintenance therapy (EWALL backbone); allogeneic HSCT with RIC regimen was allowed in fit patients in CR1 according to physician’s criteria.
Results
From 2003 to 2015, 46 patients were treated intensively vs. 32 treated semi-intensively. Except for age (intensive: 58[55-65] yr. vs. semi-intenive: 61 [56-65], p=0.01), the main clinical and hematological characteristics at baseline were comparable in the two groups. Death in induction and relapse rate were higher in the semi-intensive group, with a trend for a lower CR duration in this group. However, the OS probability was not significantly different in the two groups (Table 1). The rate of HSCT realization in CR1 was low in both groups (8% vs. 5%).
Conclusion
This study confirms the poor prognosis of older adults (55-65 yr.) with Ph-negative ALL, regardless of the intensity of the therapy. The low rate of HSCT in CR1 in this age group and a high rate of death in consolidation in patients treated intensively are of note. The trend for a significantly better CR duration in patients treated intensively did not translate into improved OS. Better therapies are needed in this age group of Ph-negative ALL patients. Supported in part with the grants PI10/01417 from Fondo de Investigaciones Sanitarias and RD12/0036/0029 from RTICC, Instituto Carlos III and 2014SGR225(GRE), Generalitat de Catalunya, Spain, and a grant from “La Caixa” Foundation.
Session topic: E-poster
Keyword(s): Acute lymphoblastic leukemia, Old, Prognosis, Treatment
{{ help_message }}
{{filter}}