
Division of Hematology

Contributions
Type: Oral Presentation
Presentation during EHA20: From 13.06.2015 15:45 to 13.06.2015 16:00
Location: Room C2
Background
Survival in acute myeloid leukemia (AML) is increasing, but most survival data come from clinical trials. National registries provide population-based survival data. Relative survival ratios (RSRs) provide a measure of total excess mortality associated with AML irrespective of whether the excess mortality is directly or indirectly because of AML. A new statistical method, loss in expectation of life (LEL), has recently been developed and provides an alternative for presenting survival.
Aims
We previously evaluated RSRs in Swedish AML patients 1973 -2005 and found a large improvement in survival for younger patients, while less improvement was seen among those 71+ years.1 We now extend the study to include patients diagnosed -2011 aiming to investigate whether there was a continuous improvement in survival and whether any improvement was seen among elderly. The aim was also to present trends in survival using LEL.
1 Derolf et al, Blood 2009
Methods
AML patients in the Swedish Cancer Registry 1973-2011 were included. Date of death was obtained from the Register of Causes of Death. RSRs and LEL were used to quantify survival. RSR is defined as the all-cause survival of the patients under study divided by the expected survival of a comparable group from the general population. LEL is calculated by subtracting the life expectancy for a patient from the life expectancy of a matched subset of the general population. This is interpreted as the number of life years lost due to an AML diagnosis. 5-year conditional LEL measures the LEL for patients conditional on the fact that they have survived 5 years since diagnosis.
Results
11598 AML patients (51% males; 2212 diagnosed 2006-2011) were included. Median age was 69 years. 10 and 69 allogeneic SCTs were perfomed in patients 61-70 years (EBMT register data) in the two last calendar periods, respectively.
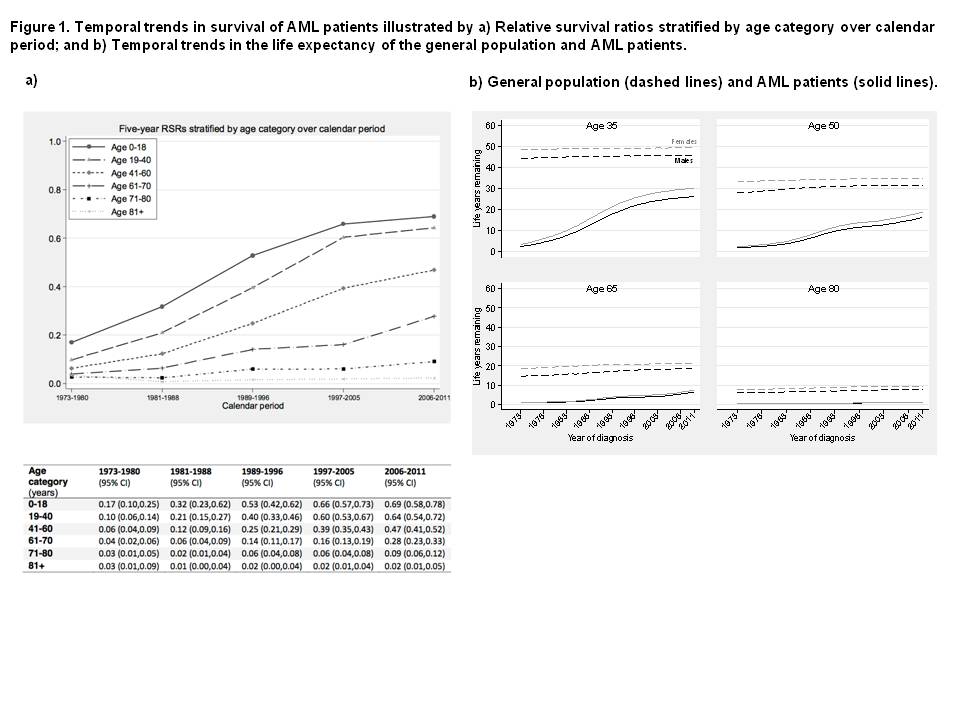
The increase in RSRs for 1973-2005 continued into the additional 6 years for all ages except patients 81+ years (Figure 1). The increase was most pronounced for patients 61-70 years; 0.16 (95% CI: 0.13-0.19) and 0.28 (95% CI: 0.23-0.33) in 1997-2005 and 2006-2011, respectively. Among patients 41-60 years RSRs increased from 0.39 (95% CI 0.35-0.43) to 0.47 (95% CI 0.41-0.52).
The greatest improvement in survival 1973-2005 was seen among patients ≤40 years; now the increase in survival was modest.
LEL decreased for all AML patients 1973-2011 but most for those aged 35 and 50 years (Figure 1). A 35-year old male diagnosed in 1973 lost, on average, 41.6 (95%CI: 40.7-42.5) life years whereas a 35-year old male diagnosed in 2011 is predicted to lose 19.5 (95%CI: 16.4-22.5) life years. 5-year conditional LEL decreased for younger patients during the study period suggesting less long-term complications of applied treatment and fewer relapses. However, young patients surviving 5 years still have their lives shortened by about two years.
Summary
AML survival continued to improve except among patients 81+ years. Most improvement was seen among patients 61-70 years. In Sweden at least 85% of patients of this age are treated with induction chemotherapy. Our results suggest clear benefit from intensive treatment including allogenic SCT. Posakonazol profylaxis was introduced during the last calendar period and risk stratification has improved, both are factors that may also contribute to increased survival in all age groups.
RSR is useful for comparisons of survival but we believe that using the LEL and comparing survival in terms of years, rather than proportions, is more intuitive and useful for communicating survival statistics.
Keyword(s): Acute myeloid leukemia, Population, Survival
Session topic: AML outcome and clinical trials
Type: Oral Presentation
Presentation during EHA20: From 13.06.2015 15:45 to 13.06.2015 16:00
Location: Room C2
Background
Survival in acute myeloid leukemia (AML) is increasing, but most survival data come from clinical trials. National registries provide population-based survival data. Relative survival ratios (RSRs) provide a measure of total excess mortality associated with AML irrespective of whether the excess mortality is directly or indirectly because of AML. A new statistical method, loss in expectation of life (LEL), has recently been developed and provides an alternative for presenting survival.
Aims
We previously evaluated RSRs in Swedish AML patients 1973 -2005 and found a large improvement in survival for younger patients, while less improvement was seen among those 71+ years.1 We now extend the study to include patients diagnosed -2011 aiming to investigate whether there was a continuous improvement in survival and whether any improvement was seen among elderly. The aim was also to present trends in survival using LEL.
1 Derolf et al, Blood 2009
Methods
AML patients in the Swedish Cancer Registry 1973-2011 were included. Date of death was obtained from the Register of Causes of Death. RSRs and LEL were used to quantify survival. RSR is defined as the all-cause survival of the patients under study divided by the expected survival of a comparable group from the general population. LEL is calculated by subtracting the life expectancy for a patient from the life expectancy of a matched subset of the general population. This is interpreted as the number of life years lost due to an AML diagnosis. 5-year conditional LEL measures the LEL for patients conditional on the fact that they have survived 5 years since diagnosis.
Results
11598 AML patients (51% males; 2212 diagnosed 2006-2011) were included. Median age was 69 years. 10 and 69 allogeneic SCTs were perfomed in patients 61-70 years (EBMT register data) in the two last calendar periods, respectively.
The increase in RSRs for 1973-2005 continued into the additional 6 years for all ages except patients 81+ years (Figure 1). The increase was most pronounced for patients 61-70 years; 0.16 (95% CI: 0.13-0.19) and 0.28 (95% CI: 0.23-0.33) in 1997-2005 and 2006-2011, respectively. Among patients 41-60 years RSRs increased from 0.39 (95% CI 0.35-0.43) to 0.47 (95% CI 0.41-0.52).
The greatest improvement in survival 1973-2005 was seen among patients ≤40 years; now the increase in survival was modest.
LEL decreased for all AML patients 1973-2011 but most for those aged 35 and 50 years (Figure 1). A 35-year old male diagnosed in 1973 lost, on average, 41.6 (95%CI: 40.7-42.5) life years whereas a 35-year old male diagnosed in 2011 is predicted to lose 19.5 (95%CI: 16.4-22.5) life years. 5-year conditional LEL decreased for younger patients during the study period suggesting less long-term complications of applied treatment and fewer relapses. However, young patients surviving 5 years still have their lives shortened by about two years.
Summary
AML survival continued to improve except among patients 81+ years. Most improvement was seen among patients 61-70 years. In Sweden at least 85% of patients of this age are treated with induction chemotherapy. Our results suggest clear benefit from intensive treatment including allogenic SCT. Posakonazol profylaxis was introduced during the last calendar period and risk stratification has improved, both are factors that may also contribute to increased survival in all age groups.
RSR is useful for comparisons of survival but we believe that using the LEL and comparing survival in terms of years, rather than proportions, is more intuitive and useful for communicating survival statistics.
Keyword(s): Acute myeloid leukemia, Population, Survival
Session topic: AML outcome and clinical trials