
Clinical Haematology, Haemato-Oncology and Bone Marrow ( Stem Cell) Transplantation

Contributions
Type: Publication Only
Background
Cytogenetic findings are important in predicting prognosis; and are an obligatory tool in stratifying patients for treatment assignment in ALL. The large studies in ALL have reported between 10-30% of cytogenetic failure. The impact of cytogenetic failure on treatment outcomes in this group with ALL has not been sufficiently explored.
Aims
To determine the differences in clinical features and treatment outcomes in patients with ALL based on the success of karyotype analyses.
Methods
We undertook a retrospective study to evaluate the impact of cytogenetic failure on treatment outcomes in patients with a diagnosis of ALL (Burkitt- excluded) treated at our tertiary care center from January 2009 till December 2014. Cytogenetic failure was used to define analyses that could not be performed in the laboratory due to no mitoses or non-informative morphology. Risk stratification and treatment was based on the BFM95 protocol for patients’ ≤15 years and GMALL in the older patients. Standard of care diagnostic tests and supportive care was administered to all patients. The cytogenetic data was retrieved from the original reports of the laboratory performing the analyses at our centre. Only cytogenetic studies sent to the laboratory were included for analyses. Clinical details were ascertained through patient admission records and discharge cards. The collected data was analyzed using SPSS.
Results
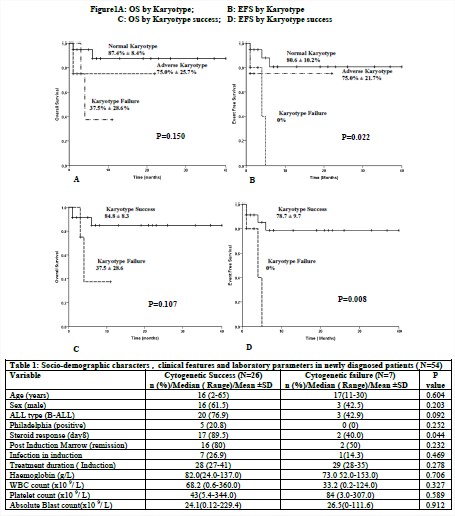
A total of 76 admitted patients were diagnosed with ALL. Of these 54 (71.1%) continued with treatment. Bone marrow was sent for cytogenetic analyses in 33 of these patients. There were no significant differences observed in terms of socio-demographic and baseline laboratory parameters among the two groups based on the success of cytogenetic analyses (table1).The Event Free Survival (EFS) and Overall Survival (OS) were lesser in patients with cytogenetic failure than in those who had a successful karyotype analyses (Figure 1). With a mean follow up of 32 months, the EFS at one year in those with cytogenetic failure was significantly lower than those with a successful karyotype analyses (p=0.008). When compared against the outcomes of patients with adverse karyotype (t (9; 22) or >3 abnormalities), those with cytogenetic failure had a significantly lower EFS (p=0.022).
Summary
Risk stratification in ALL has not defined the optimal strategy in patients with cytogenetic failure. Unsuccessful cytogenetics likely predicts a poor outcome. This needs to be further explored by facilitating the inclusion of these patients as a group in clinical trials.
Keyword(s): ALL, Cytogenetics, Prognosis
Session topic: Publication Only
Type: Publication Only
Background
Cytogenetic findings are important in predicting prognosis; and are an obligatory tool in stratifying patients for treatment assignment in ALL. The large studies in ALL have reported between 10-30% of cytogenetic failure. The impact of cytogenetic failure on treatment outcomes in this group with ALL has not been sufficiently explored.
Aims
To determine the differences in clinical features and treatment outcomes in patients with ALL based on the success of karyotype analyses.
Methods
We undertook a retrospective study to evaluate the impact of cytogenetic failure on treatment outcomes in patients with a diagnosis of ALL (Burkitt- excluded) treated at our tertiary care center from January 2009 till December 2014. Cytogenetic failure was used to define analyses that could not be performed in the laboratory due to no mitoses or non-informative morphology. Risk stratification and treatment was based on the BFM95 protocol for patients’ ≤15 years and GMALL in the older patients. Standard of care diagnostic tests and supportive care was administered to all patients. The cytogenetic data was retrieved from the original reports of the laboratory performing the analyses at our centre. Only cytogenetic studies sent to the laboratory were included for analyses. Clinical details were ascertained through patient admission records and discharge cards. The collected data was analyzed using SPSS.
Results
A total of 76 admitted patients were diagnosed with ALL. Of these 54 (71.1%) continued with treatment. Bone marrow was sent for cytogenetic analyses in 33 of these patients. There were no significant differences observed in terms of socio-demographic and baseline laboratory parameters among the two groups based on the success of cytogenetic analyses (table1).The Event Free Survival (EFS) and Overall Survival (OS) were lesser in patients with cytogenetic failure than in those who had a successful karyotype analyses (Figure 1). With a mean follow up of 32 months, the EFS at one year in those with cytogenetic failure was significantly lower than those with a successful karyotype analyses (p=0.008). When compared against the outcomes of patients with adverse karyotype (t (9; 22) or >3 abnormalities), those with cytogenetic failure had a significantly lower EFS (p=0.022).
Summary
Risk stratification in ALL has not defined the optimal strategy in patients with cytogenetic failure. Unsuccessful cytogenetics likely predicts a poor outcome. This needs to be further explored by facilitating the inclusion of these patients as a group in clinical trials.
Keyword(s): ALL, Cytogenetics, Prognosis
Session topic: Publication Only