

Contributions
Type: Publication Only
Background
Myeloid Sarcoma (MS) is a rare neoplasm composed of immature myeloid cells potentially occurring in any extramedullary organ, most commonly in the lymph node and soft tissues. MS develops before, concurrently or after the diagnosis of acute myeloid leukemia (AML), but can rarely occur without bone marrow infiltration by leukemia. MS is associated with poor outcome. The rarity of this presentation has been an obstacle to characterize its clinical features and prognosis.
Aims
The aim of the study was to analyze characteristics, treatments and overall survival of all patients presenting with MS.
Methods
We retrospectively reviewed medical record of patients who presented with MS to our institute from 2004 through 2015. In total 28 patients with MS were identified.
Results
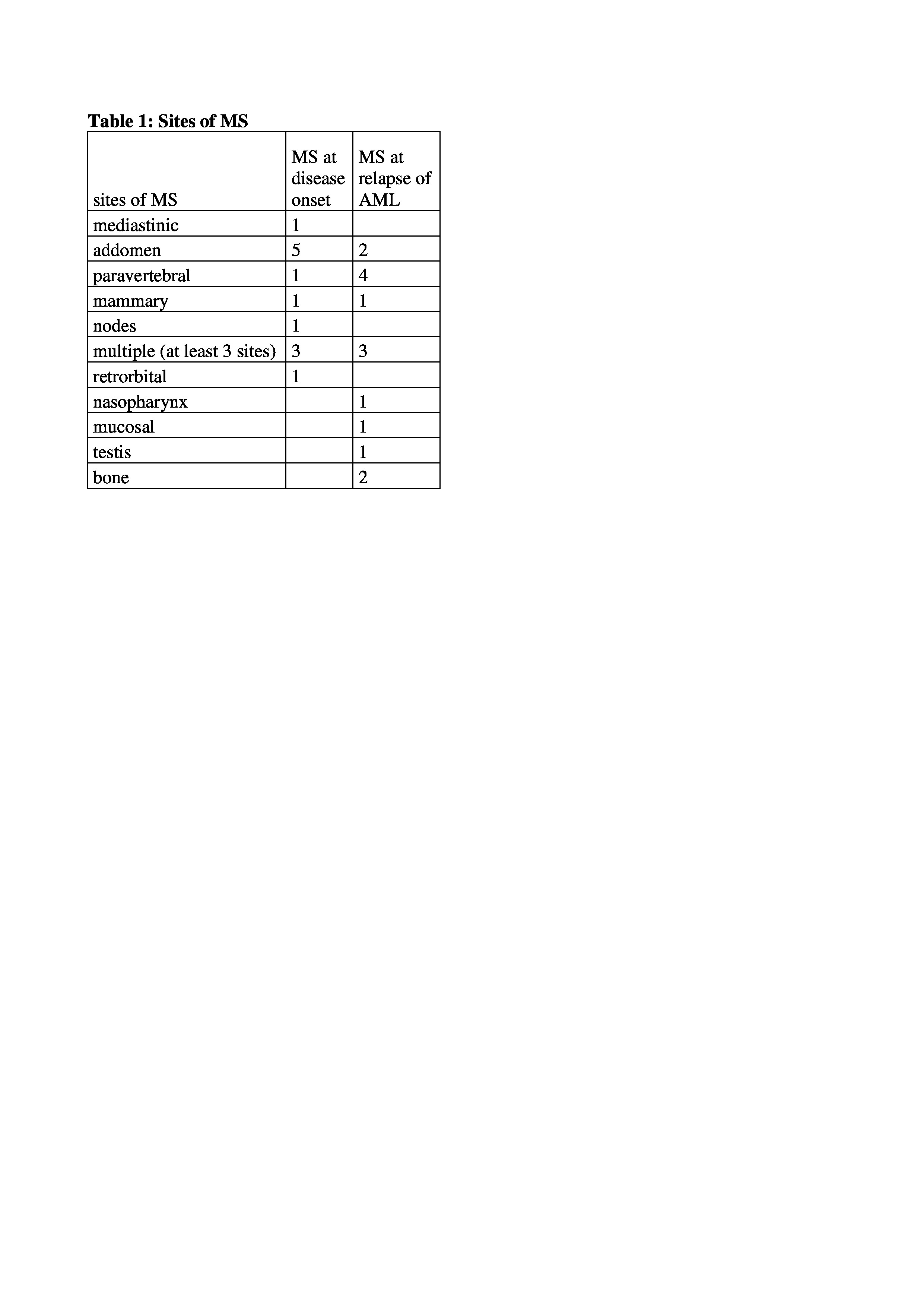
Thirteen patients had a MS at disease onset, 2 as primary sarcoma and 11 associated with AML, 15 developed MS at relapse of AML, 9 patients had only extramedullary relapse (EM), 6 also bone marrow involvement (table 1). The median age of patients at MS presentation was 45 years (range 22-76).
The most commonly involved site for patients with MS at disease onset was abdomen (gastrointestinal tract and kidney.) Six out of 13 patients had cytogenetic abnormalities involving chromosomes 8, 21, 16, Y; karyotype was normal in 3/13 and complex in 2/13. Cytogenetic was not available in 2/13 cases.
Eleven out of 13 patients with MS at diagnosis received allogeneic stem cells transplantation (alloSCT) as post-remission treatment and 2 patients were treated with palliative chemotherapy due to old age. After a median follow-up of 560 days (range 108-3715) 8/13 patients (61%) are alive and 6/13 (46%) are disease free.
Among the 15 patients who have developed a MS at AML relapse the most frequent location was paravertebral (table 1) The median age at presentation was 46 years (range 22-65). Seven out of 13 available cytogenetic analysis were normal, 5 complex and 1 was t(8;21) plus delY.
The median time from AML diagnosis to EM relapse was 657 days (range 308-2312) and in 14/15 cases EM occurred after alloSCT, with a median time to relapse of 444 days (range 254-3195).
Salvage treatment of these patients: 6 alloSCT, 3 immunotherapy, 4 chemotherapy, 2 palliative radiotherapy.
At last follow up three out of 15 patients (20%) are alive and in complete remission from AML and MS (median follow-up was 350 days, range 39-1847).
Summary
With this study we provide a single institution experience of MS management and outcome. Our Institution is a referral centre for alloSCT thus explaining the high rate of alloSCT in this series. Our data support alloSCT as part of first line treatment of MS after chemotherapy. EM relapse of AML after first line therapy has a poor prognosis even after intensive treatment. The high rate of EM relapse after alloSCT (14/15) suggests that MS may represent a form of post alloSCT AML immune escape not necessary related to sarcomatous presentation at onset. Larger multicenter studies are needed to better and more fully assess outcomes of these patients.
Session topic: Publication Only
Type: Publication Only
Background
Myeloid Sarcoma (MS) is a rare neoplasm composed of immature myeloid cells potentially occurring in any extramedullary organ, most commonly in the lymph node and soft tissues. MS develops before, concurrently or after the diagnosis of acute myeloid leukemia (AML), but can rarely occur without bone marrow infiltration by leukemia. MS is associated with poor outcome. The rarity of this presentation has been an obstacle to characterize its clinical features and prognosis.
Aims
The aim of the study was to analyze characteristics, treatments and overall survival of all patients presenting with MS.
Methods
We retrospectively reviewed medical record of patients who presented with MS to our institute from 2004 through 2015. In total 28 patients with MS were identified.
Results
Thirteen patients had a MS at disease onset, 2 as primary sarcoma and 11 associated with AML, 15 developed MS at relapse of AML, 9 patients had only extramedullary relapse (EM), 6 also bone marrow involvement (table 1). The median age of patients at MS presentation was 45 years (range 22-76).
The most commonly involved site for patients with MS at disease onset was abdomen (gastrointestinal tract and kidney.) Six out of 13 patients had cytogenetic abnormalities involving chromosomes 8, 21, 16, Y; karyotype was normal in 3/13 and complex in 2/13. Cytogenetic was not available in 2/13 cases.
Eleven out of 13 patients with MS at diagnosis received allogeneic stem cells transplantation (alloSCT) as post-remission treatment and 2 patients were treated with palliative chemotherapy due to old age. After a median follow-up of 560 days (range 108-3715) 8/13 patients (61%) are alive and 6/13 (46%) are disease free.
Among the 15 patients who have developed a MS at AML relapse the most frequent location was paravertebral (table 1) The median age at presentation was 46 years (range 22-65). Seven out of 13 available cytogenetic analysis were normal, 5 complex and 1 was t(8;21) plus delY.
The median time from AML diagnosis to EM relapse was 657 days (range 308-2312) and in 14/15 cases EM occurred after alloSCT, with a median time to relapse of 444 days (range 254-3195).
Salvage treatment of these patients: 6 alloSCT, 3 immunotherapy, 4 chemotherapy, 2 palliative radiotherapy.
At last follow up three out of 15 patients (20%) are alive and in complete remission from AML and MS (median follow-up was 350 days, range 39-1847).
Summary
With this study we provide a single institution experience of MS management and outcome. Our Institution is a referral centre for alloSCT thus explaining the high rate of alloSCT in this series. Our data support alloSCT as part of first line treatment of MS after chemotherapy. EM relapse of AML after first line therapy has a poor prognosis even after intensive treatment. The high rate of EM relapse after alloSCT (14/15) suggests that MS may represent a form of post alloSCT AML immune escape not necessary related to sarcomatous presentation at onset. Larger multicenter studies are needed to better and more fully assess outcomes of these patients.
Session topic: Publication Only