
A MULTICENTER, RETROSPECTIVE ANALYSIS OF LOW-GRADE PRIMARY FOLLICULAR LYMPHOMA OF THE GASTROINTESTINAL TRACT: TREATMENT AND OUTCOME
(Abstract release date: 05/21/15)
EHA Library. Lee J. 06/12/15; 102968; PB1790
Disclosure(s): Severance hospitalInternal medicine

Dr. Jung Yeon Lee
Contributions
Contributions
Abstract
Abstract: PB1790
Type: Publication Only
Background
Primary gastrointestinal (GI) follicular lymphoma (FL) has been regarded as a relatively rare malignant disease, accounting for 1-3.6% of primary non-Hodgkin lymphomas of the GI tract. The primary FL of the GI tract occurs most often in middle-aged adults with a 2:1 female predominance. The most frequent primary occurrence location is duodenum. The low-grade primary FL of the GI tract which is especially located at duodenum characterized as an indolent. Although the various therapeutic strategies have been developed for FL, there is no definite guideline for the treatment of low-grade primary FL of the GI tract.
Aims
In this study, we analyzed our experience of low-grade primary FL of the GI tract according to the treatments.
Methods
A total of 12 patients who diagnosed as a low-grade primary FL of the GI tract between June 2005 and June 2014 from 5 institutions in Korea were retrospectively analyzed. Low-grade primary FL of the GI tract was defined as Lugano stage I or II and WHO histologic grade 1 or 2. Endoscopy and immunohistochemical pathologic work-up were performed at diagnosis. The patients were classified according to the treatment strategies such as watch & wait group (n=4) and treatment group (n=8). Treatments included various chemotherapies (CTx) and radiotherapy (RTx).
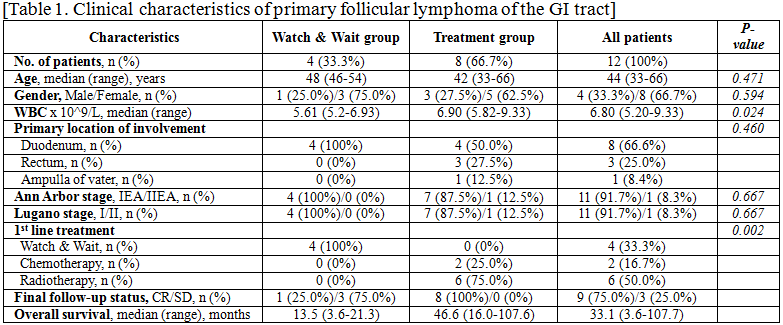
Results
Median age was 44 years (range, 33-66) and a female predominance was observed (male:female = 4:8). All patients had an Eastern Cooperative Oncology Group (ECOG) performance score of 0 or 1. The most common reason for initial evaluations of primary FL of the GI tract was health screening (n=10, 83.3%). Only two patients received initial evaluations due to GI symptoms. The small intestine, especially the 2nd or 3rd portion of duodenum was the most common primary site of involvement (n=8, 66.6%). There were similar clinical characteristics between the two groups. Exceptionally, white blood cell (WBC) count (P=0.024) at diagnosis was higher in the treatment group. The primary site of involvement was not different between the two groups. However, the only primary site of the watch & wait group was duodenum (n=4, 100%). In the watch & wait group, the maintenance of stable disease status was observed in all patients. However, one patient in the watch & wait group eventually received additional RTx after the initial observational period of 19.4 months according to the decision of the attending physician. In the treatment group, two patients received CTx such as CVP (cyclophosphamide, vincristine and prednisone, n=1) or CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone, n=1) and six patients received RTx (median 3600 cGy, range, 2520-4140). These eight patients in the treatment group achieved complete remission (CR) after treatment, but one patient with low-grade primary FL of the rectum who received 6th cycles of CVP CTx relapsed at 30.5 months after achieving 1st CR. She received 4 cycles of weekly rituximab monotherapy and re-achieved CR. After a median follow-up of 33.1 months (range, 3.6 to 107.7 months), all 12 patients were alive.
Summary
In this study, we confirmed that the watch & wait strategy was safe in low-grade primary FL of duodenum. In addition, radiation alone also was an appropriate strategy for the low-grade primary FL of the GI tract. However, close monitoring would be necessary for the patients with non-duodenal site of the low-grade primary FL. Further studies with more patients would be needed to confirm appropriate treatment strategies for the low-grade primary FL of the GI tract.
Keyword(s): Follicular lymphoma, Outcome, Treatment
Session topic: Publication Only
Type: Publication Only
Background
Primary gastrointestinal (GI) follicular lymphoma (FL) has been regarded as a relatively rare malignant disease, accounting for 1-3.6% of primary non-Hodgkin lymphomas of the GI tract. The primary FL of the GI tract occurs most often in middle-aged adults with a 2:1 female predominance. The most frequent primary occurrence location is duodenum. The low-grade primary FL of the GI tract which is especially located at duodenum characterized as an indolent. Although the various therapeutic strategies have been developed for FL, there is no definite guideline for the treatment of low-grade primary FL of the GI tract.
Aims
In this study, we analyzed our experience of low-grade primary FL of the GI tract according to the treatments.
Methods
A total of 12 patients who diagnosed as a low-grade primary FL of the GI tract between June 2005 and June 2014 from 5 institutions in Korea were retrospectively analyzed. Low-grade primary FL of the GI tract was defined as Lugano stage I or II and WHO histologic grade 1 or 2. Endoscopy and immunohistochemical pathologic work-up were performed at diagnosis. The patients were classified according to the treatment strategies such as watch & wait group (n=4) and treatment group (n=8). Treatments included various chemotherapies (CTx) and radiotherapy (RTx).
Results
Median age was 44 years (range, 33-66) and a female predominance was observed (male:female = 4:8). All patients had an Eastern Cooperative Oncology Group (ECOG) performance score of 0 or 1. The most common reason for initial evaluations of primary FL of the GI tract was health screening (n=10, 83.3%). Only two patients received initial evaluations due to GI symptoms. The small intestine, especially the 2nd or 3rd portion of duodenum was the most common primary site of involvement (n=8, 66.6%). There were similar clinical characteristics between the two groups. Exceptionally, white blood cell (WBC) count (P=0.024) at diagnosis was higher in the treatment group. The primary site of involvement was not different between the two groups. However, the only primary site of the watch & wait group was duodenum (n=4, 100%). In the watch & wait group, the maintenance of stable disease status was observed in all patients. However, one patient in the watch & wait group eventually received additional RTx after the initial observational period of 19.4 months according to the decision of the attending physician. In the treatment group, two patients received CTx such as CVP (cyclophosphamide, vincristine and prednisone, n=1) or CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone, n=1) and six patients received RTx (median 3600 cGy, range, 2520-4140). These eight patients in the treatment group achieved complete remission (CR) after treatment, but one patient with low-grade primary FL of the rectum who received 6th cycles of CVP CTx relapsed at 30.5 months after achieving 1st CR. She received 4 cycles of weekly rituximab monotherapy and re-achieved CR. After a median follow-up of 33.1 months (range, 3.6 to 107.7 months), all 12 patients were alive.
Summary
In this study, we confirmed that the watch & wait strategy was safe in low-grade primary FL of duodenum. In addition, radiation alone also was an appropriate strategy for the low-grade primary FL of the GI tract. However, close monitoring would be necessary for the patients with non-duodenal site of the low-grade primary FL. Further studies with more patients would be needed to confirm appropriate treatment strategies for the low-grade primary FL of the GI tract.
Keyword(s): Follicular lymphoma, Outcome, Treatment
Session topic: Publication Only
Abstract: PB1790
Type: Publication Only
Background
Primary gastrointestinal (GI) follicular lymphoma (FL) has been regarded as a relatively rare malignant disease, accounting for 1-3.6% of primary non-Hodgkin lymphomas of the GI tract. The primary FL of the GI tract occurs most often in middle-aged adults with a 2:1 female predominance. The most frequent primary occurrence location is duodenum. The low-grade primary FL of the GI tract which is especially located at duodenum characterized as an indolent. Although the various therapeutic strategies have been developed for FL, there is no definite guideline for the treatment of low-grade primary FL of the GI tract.
Aims
In this study, we analyzed our experience of low-grade primary FL of the GI tract according to the treatments.
Methods
A total of 12 patients who diagnosed as a low-grade primary FL of the GI tract between June 2005 and June 2014 from 5 institutions in Korea were retrospectively analyzed. Low-grade primary FL of the GI tract was defined as Lugano stage I or II and WHO histologic grade 1 or 2. Endoscopy and immunohistochemical pathologic work-up were performed at diagnosis. The patients were classified according to the treatment strategies such as watch & wait group (n=4) and treatment group (n=8). Treatments included various chemotherapies (CTx) and radiotherapy (RTx).
Results
Median age was 44 years (range, 33-66) and a female predominance was observed (male:female = 4:8). All patients had an Eastern Cooperative Oncology Group (ECOG) performance score of 0 or 1. The most common reason for initial evaluations of primary FL of the GI tract was health screening (n=10, 83.3%). Only two patients received initial evaluations due to GI symptoms. The small intestine, especially the 2nd or 3rd portion of duodenum was the most common primary site of involvement (n=8, 66.6%). There were similar clinical characteristics between the two groups. Exceptionally, white blood cell (WBC) count (P=0.024) at diagnosis was higher in the treatment group. The primary site of involvement was not different between the two groups. However, the only primary site of the watch & wait group was duodenum (n=4, 100%). In the watch & wait group, the maintenance of stable disease status was observed in all patients. However, one patient in the watch & wait group eventually received additional RTx after the initial observational period of 19.4 months according to the decision of the attending physician. In the treatment group, two patients received CTx such as CVP (cyclophosphamide, vincristine and prednisone, n=1) or CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone, n=1) and six patients received RTx (median 3600 cGy, range, 2520-4140). These eight patients in the treatment group achieved complete remission (CR) after treatment, but one patient with low-grade primary FL of the rectum who received 6th cycles of CVP CTx relapsed at 30.5 months after achieving 1st CR. She received 4 cycles of weekly rituximab monotherapy and re-achieved CR. After a median follow-up of 33.1 months (range, 3.6 to 107.7 months), all 12 patients were alive.
Summary
In this study, we confirmed that the watch & wait strategy was safe in low-grade primary FL of duodenum. In addition, radiation alone also was an appropriate strategy for the low-grade primary FL of the GI tract. However, close monitoring would be necessary for the patients with non-duodenal site of the low-grade primary FL. Further studies with more patients would be needed to confirm appropriate treatment strategies for the low-grade primary FL of the GI tract.
Keyword(s): Follicular lymphoma, Outcome, Treatment
Session topic: Publication Only
Type: Publication Only
Background
Primary gastrointestinal (GI) follicular lymphoma (FL) has been regarded as a relatively rare malignant disease, accounting for 1-3.6% of primary non-Hodgkin lymphomas of the GI tract. The primary FL of the GI tract occurs most often in middle-aged adults with a 2:1 female predominance. The most frequent primary occurrence location is duodenum. The low-grade primary FL of the GI tract which is especially located at duodenum characterized as an indolent. Although the various therapeutic strategies have been developed for FL, there is no definite guideline for the treatment of low-grade primary FL of the GI tract.
Aims
In this study, we analyzed our experience of low-grade primary FL of the GI tract according to the treatments.
Methods
A total of 12 patients who diagnosed as a low-grade primary FL of the GI tract between June 2005 and June 2014 from 5 institutions in Korea were retrospectively analyzed. Low-grade primary FL of the GI tract was defined as Lugano stage I or II and WHO histologic grade 1 or 2. Endoscopy and immunohistochemical pathologic work-up were performed at diagnosis. The patients were classified according to the treatment strategies such as watch & wait group (n=4) and treatment group (n=8). Treatments included various chemotherapies (CTx) and radiotherapy (RTx).
Results
Median age was 44 years (range, 33-66) and a female predominance was observed (male:female = 4:8). All patients had an Eastern Cooperative Oncology Group (ECOG) performance score of 0 or 1. The most common reason for initial evaluations of primary FL of the GI tract was health screening (n=10, 83.3%). Only two patients received initial evaluations due to GI symptoms. The small intestine, especially the 2nd or 3rd portion of duodenum was the most common primary site of involvement (n=8, 66.6%). There were similar clinical characteristics between the two groups. Exceptionally, white blood cell (WBC) count (P=0.024) at diagnosis was higher in the treatment group. The primary site of involvement was not different between the two groups. However, the only primary site of the watch & wait group was duodenum (n=4, 100%). In the watch & wait group, the maintenance of stable disease status was observed in all patients. However, one patient in the watch & wait group eventually received additional RTx after the initial observational period of 19.4 months according to the decision of the attending physician. In the treatment group, two patients received CTx such as CVP (cyclophosphamide, vincristine and prednisone, n=1) or CHOP (cyclophosphamide, doxorubicin, vincristine and prednisone, n=1) and six patients received RTx (median 3600 cGy, range, 2520-4140). These eight patients in the treatment group achieved complete remission (CR) after treatment, but one patient with low-grade primary FL of the rectum who received 6th cycles of CVP CTx relapsed at 30.5 months after achieving 1st CR. She received 4 cycles of weekly rituximab monotherapy and re-achieved CR. After a median follow-up of 33.1 months (range, 3.6 to 107.7 months), all 12 patients were alive.
Summary
In this study, we confirmed that the watch & wait strategy was safe in low-grade primary FL of duodenum. In addition, radiation alone also was an appropriate strategy for the low-grade primary FL of the GI tract. However, close monitoring would be necessary for the patients with non-duodenal site of the low-grade primary FL. Further studies with more patients would be needed to confirm appropriate treatment strategies for the low-grade primary FL of the GI tract.
Keyword(s): Follicular lymphoma, Outcome, Treatment
Session topic: Publication Only
{{ help_message }}
{{filter}}