
Hematology

Contributions
Type: Publication Only
Background
Gastric mucosa-associated lymphoid tissue (MALT) B-cell lymphoma represents the most frequent localization of extranodal marginal-zone lymphoma (MZL), characterized by a well established association with Helicobacter pylori (HP) infection. The first-line treatment for HP positive patients is HP eradication therapy; however, there is no consensus on the standard management for patients with HP negative or persistent disease after HP eradication. Current approaches include radiation therapy, chemotherapy and immunotherapy with rituximab, either alone or in combination. Despite the activity of many alkylating agents and nucleoside analogues against MALT lymphoma, evidence about the superiority of a specific regimen toward others is still lacking.
Aims
in this study we have investigated long-term efficacy and safety of fludarabine and mitoxantrone in association with rituximab (R-FM) as first-line treatment for gastric MALT lymphoma with HP negative or persistent disease after HP eradication.
Methods
A cohort of 13 patients (M/F: 5/8; median age 65 yrs) diagnosed with gastric MALT lymphoma by gastroscopy biopsies and treated between August 2005 and March 2012 was retrospectively analyzed. All patients completed staging with whole body CT scan and bone marrow (BM) biopsy. Five patients had stage I disease, 7 stage II and 1 stage IV, HP was positive in 9/13 patients. Induction treatment consisted of fludarabine (25mg/m2 i.v. on days 2 to 4), mitoxantrone (10mg/m2 i.v. on day 2) and rituximab (375 mg/m2 i.v. on day 1), administered for up to 6 cycles every 28 days. Final response assessment including esophagogastroduodenoscopy with random biopsies and CT scan was done 4-6 weeks after completion of therapy according to the 2007 Revised Response Criteria. During follow-up period CT scan was performed together with esophagogastroduodenoscopy every 6 months for the first 2 years (annually for stage I patients). Thereafter, endoscopy was performed annually until the 5th year, after this period the patients continued only clinical follow-up.
Results
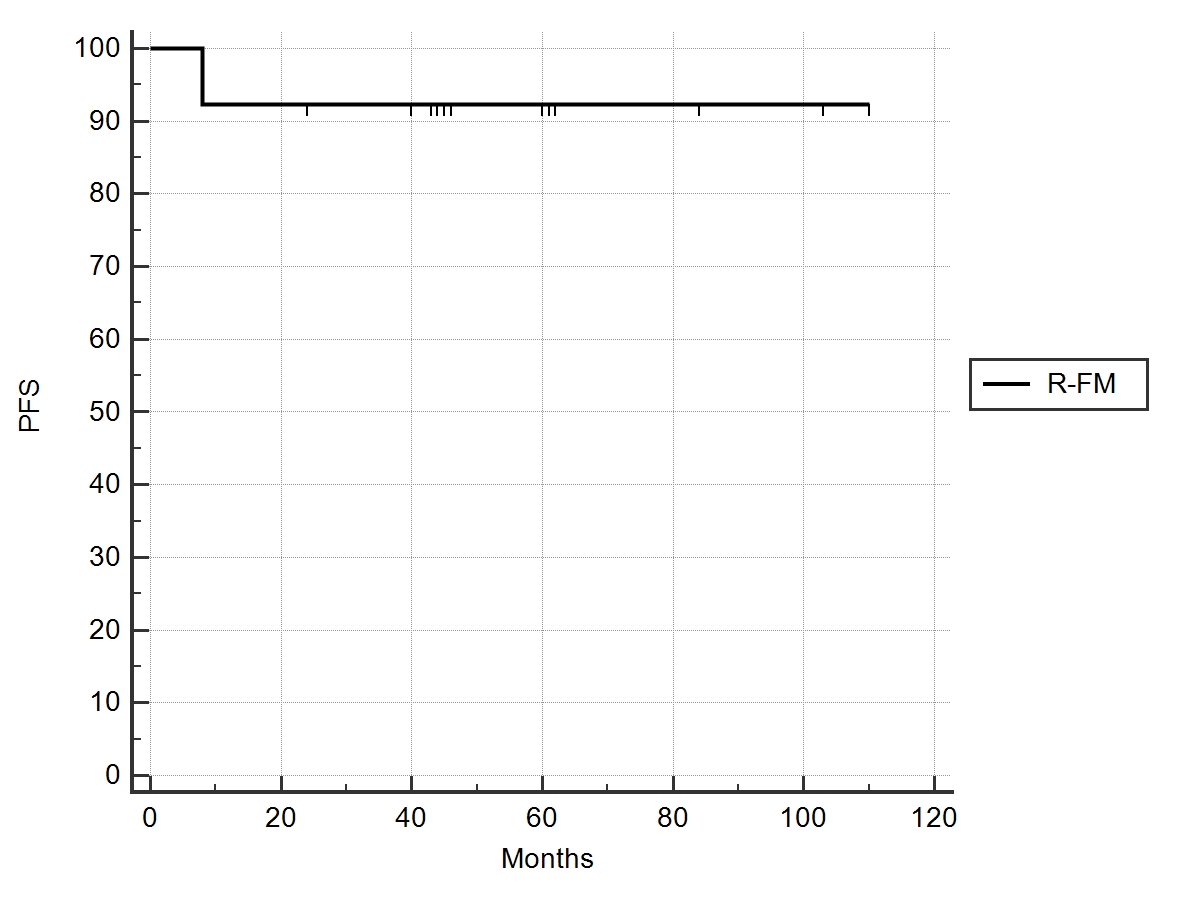
All patients (13/13, 100%) achieved a complete remission (CR), a median of 4 cycles (range 3-6) of R-FM were given and all were evaluable for response and toxicity. Treatment-related toxicities were mainly hematologic, with grade 3-4 neutropenia observed in 11/13 patients (84.6%), grade 2 thrombocytopenia and anemia in 1 and 2 patients, respectively. All but one cases required secondary neutropenia prophylaxis with filgrastim, 1 patient had grade 3 febrile neutropenia. The same patient was hospitalized while on treatment because of non-neutropenic fever with detection of Candida Albicans by stool culture; 2 months later experienced CMV reactivation, too. Two patients developed prolonged pancytopenia, with slow recovery after about 12 months. Grade II nausea was documented in 4/13 patients, no other adverse events occurred. After a median follow-up of 60 months (range 24-110) all patients were alive, 1/13 had disease relapse after 8 months and received total gastrectomy; estimated 9-year progression-free survival and overall survival were 92.4% (Fig.1) and 100%, respectively.
Summary
This small series of homogeneously treated patients suggests R-FM regimen has a high long-term efficacy as frontline treatment for gastric MALT lymphoma. However, the high incidence of grade 3-4 hematological toxicity makes this treatment less safe compared to the previously published results of other regimens such as rituximab in combination with chlorambucil or bendamustine. It could remain a suitable option for patients with advanced-stage disease, while exluding stage I.
Keyword(s): Fludarabine, Gastric MALT lymphoma, Mitoxantrone, Rituximab
Session topic: Publication Only
Type: Publication Only
Background
Gastric mucosa-associated lymphoid tissue (MALT) B-cell lymphoma represents the most frequent localization of extranodal marginal-zone lymphoma (MZL), characterized by a well established association with Helicobacter pylori (HP) infection. The first-line treatment for HP positive patients is HP eradication therapy; however, there is no consensus on the standard management for patients with HP negative or persistent disease after HP eradication. Current approaches include radiation therapy, chemotherapy and immunotherapy with rituximab, either alone or in combination. Despite the activity of many alkylating agents and nucleoside analogues against MALT lymphoma, evidence about the superiority of a specific regimen toward others is still lacking.
Aims
in this study we have investigated long-term efficacy and safety of fludarabine and mitoxantrone in association with rituximab (R-FM) as first-line treatment for gastric MALT lymphoma with HP negative or persistent disease after HP eradication.
Methods
A cohort of 13 patients (M/F: 5/8; median age 65 yrs) diagnosed with gastric MALT lymphoma by gastroscopy biopsies and treated between August 2005 and March 2012 was retrospectively analyzed. All patients completed staging with whole body CT scan and bone marrow (BM) biopsy. Five patients had stage I disease, 7 stage II and 1 stage IV, HP was positive in 9/13 patients. Induction treatment consisted of fludarabine (25mg/m2 i.v. on days 2 to 4), mitoxantrone (10mg/m2 i.v. on day 2) and rituximab (375 mg/m2 i.v. on day 1), administered for up to 6 cycles every 28 days. Final response assessment including esophagogastroduodenoscopy with random biopsies and CT scan was done 4-6 weeks after completion of therapy according to the 2007 Revised Response Criteria. During follow-up period CT scan was performed together with esophagogastroduodenoscopy every 6 months for the first 2 years (annually for stage I patients). Thereafter, endoscopy was performed annually until the 5th year, after this period the patients continued only clinical follow-up.
Results
All patients (13/13, 100%) achieved a complete remission (CR), a median of 4 cycles (range 3-6) of R-FM were given and all were evaluable for response and toxicity. Treatment-related toxicities were mainly hematologic, with grade 3-4 neutropenia observed in 11/13 patients (84.6%), grade 2 thrombocytopenia and anemia in 1 and 2 patients, respectively. All but one cases required secondary neutropenia prophylaxis with filgrastim, 1 patient had grade 3 febrile neutropenia. The same patient was hospitalized while on treatment because of non-neutropenic fever with detection of Candida Albicans by stool culture; 2 months later experienced CMV reactivation, too. Two patients developed prolonged pancytopenia, with slow recovery after about 12 months. Grade II nausea was documented in 4/13 patients, no other adverse events occurred. After a median follow-up of 60 months (range 24-110) all patients were alive, 1/13 had disease relapse after 8 months and received total gastrectomy; estimated 9-year progression-free survival and overall survival were 92.4% (Fig.1) and 100%, respectively.
Summary
This small series of homogeneously treated patients suggests R-FM regimen has a high long-term efficacy as frontline treatment for gastric MALT lymphoma. However, the high incidence of grade 3-4 hematological toxicity makes this treatment less safe compared to the previously published results of other regimens such as rituximab in combination with chlorambucil or bendamustine. It could remain a suitable option for patients with advanced-stage disease, while exluding stage I.
Keyword(s): Fludarabine, Gastric MALT lymphoma, Mitoxantrone, Rituximab
Session topic: Publication Only