
TO THE DIFFERENTIAL DIAGNOSIS OF ACUTE MYELOBLASTIC LEUKEMIA AND CHRONIC MYELOID LEUKEMIA STARTED WITH BLAST CRISIS
(Abstract release date: 05/21/15)
EHA Library. Saralidze T. 06/12/15; 102851; PB1738

Dr. Tamar Saralidze
Contributions
Contributions
Abstract
Abstract: PB1738
Type: Publication Only
Background
Despite the achievements of modern medicine sometimes there is a problem to differentiate chronic myeloid leukemia (CML) started with blast crisis from acute myeloblastic leukemia (AML), especially in the cases of Ph chromosome negative or BCR-ABL1- negative cases. Even in the presence of this marker one should have taken in mind that there are cases of Ph + AML as well.
Aims
The aim of our study was to precise the diagnose in patients with blast cells in peripheral blood and prominent hepato- and splenomegaly suspicious on CML and reveal additional criteria for the diagnosis of CML started with blast crisis.
Methods
To solve this problem we have used peripheral blood and bone marrow cell culture method worked out by us. This method supports propagation of blast cells specific for each form and variant of leukemia and enables to reveal the malignant clone according to morphocytochemical investigation or phenotyping in vitro proliferating cells (Shvelidze, Saralidze et al. Atlas of Hematology, 2013. http://www.e-bookland.ge/Books/medical/ATLAS-of-HEMATOLOGY). We investigated peripheral blood and bone marrow cell cultures of 5 patients with CML presented with blast crisis at the time of diagnosis, 8 patients with CML at chronic stage, 2 patients with CML in accelerated phase and 7 patients with AML (3 cases of AML without maturation and 4 cases of AML with maturation).
Results
Our studies showed that in all cases of AML proliferation of blast cells is confirmed by abundance of blast cells in cultures during 2 weeks of cultivation and appearance of maturation part of them up to promyelocytes and myelocytes and rarely to the band neutrophils in late cultures. On contrary, in the cases of CML presented with blast crisis as well as in the cases of CML at chronic stage, rapid maturation of blast cells up to band neutrophils is obvious from the beginning of cultivation. Just from the second day of cultivation in cultures of patients with CML disappearance of blast cells and abundance of band and segmented granulocytes, mainly neutrophilic, but eosinophilic and basophilic also are observed (Fig. 1). It must be noticed that from 2 patients with CML in accelerated phase in one case majority of cells in culture were matured granulocytes, that is characteristic for CML, while in another case culture material was presented by abundance of immature myeloid cells – myeloblasts, promyelocytes and myelocytes and a few band and segmented granulocytes that pointed to tumor progression. In the last case treatment was not effective at all.
Summary
Results of our study show that blood and bone marrow culture data of patients with CML can be successfully used as additional criteria for the differentiation of CML started with blast crisis from AML as far as in cultures of patients with AML abundant proliferation of blast cells is observed, whereas in the cases of CML started with blast crisis rapid maturation of blast cells up to band neutrophils from the beginning of cultivation is obvious. Abundance of immature cells in blood or bone marrow cultures of patients with CML points to tumor progression in spite of the clinical stage of disease and represents a bad prognostic marker. Cytochemical study or immunophenotyping of proliferated in vitro cells can help to determine the type of new proliferative clone.
Keyword(s): Acute myeloid leukemia, Chronic myeloid leukemia, Diagnosis, In vitro expression
Session topic: Publication Only
Type: Publication Only
Background
Despite the achievements of modern medicine sometimes there is a problem to differentiate chronic myeloid leukemia (CML) started with blast crisis from acute myeloblastic leukemia (AML), especially in the cases of Ph chromosome negative or BCR-ABL1- negative cases. Even in the presence of this marker one should have taken in mind that there are cases of Ph + AML as well.
Aims
The aim of our study was to precise the diagnose in patients with blast cells in peripheral blood and prominent hepato- and splenomegaly suspicious on CML and reveal additional criteria for the diagnosis of CML started with blast crisis.
Methods
To solve this problem we have used peripheral blood and bone marrow cell culture method worked out by us. This method supports propagation of blast cells specific for each form and variant of leukemia and enables to reveal the malignant clone according to morphocytochemical investigation or phenotyping in vitro proliferating cells (Shvelidze, Saralidze et al. Atlas of Hematology, 2013. http://www.e-bookland.ge/Books/medical/ATLAS-of-HEMATOLOGY). We investigated peripheral blood and bone marrow cell cultures of 5 patients with CML presented with blast crisis at the time of diagnosis, 8 patients with CML at chronic stage, 2 patients with CML in accelerated phase and 7 patients with AML (3 cases of AML without maturation and 4 cases of AML with maturation).
Results
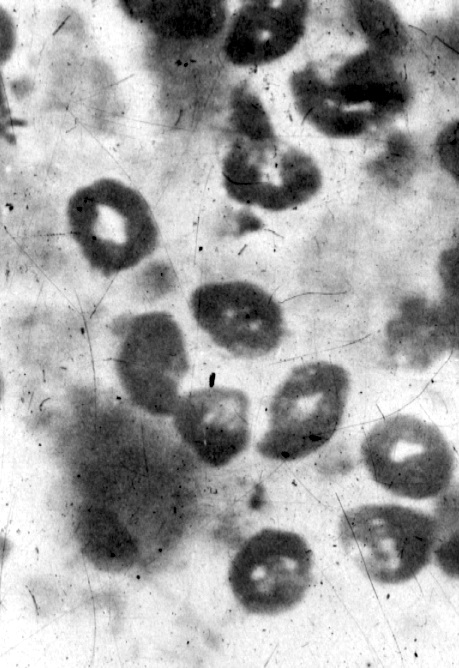
Our studies showed that in all cases of AML proliferation of blast cells is confirmed by abundance of blast cells in cultures during 2 weeks of cultivation and appearance of maturation part of them up to promyelocytes and myelocytes and rarely to the band neutrophils in late cultures. On contrary, in the cases of CML presented with blast crisis as well as in the cases of CML at chronic stage, rapid maturation of blast cells up to band neutrophils is obvious from the beginning of cultivation. Just from the second day of cultivation in cultures of patients with CML disappearance of blast cells and abundance of band and segmented granulocytes, mainly neutrophilic, but eosinophilic and basophilic also are observed (Fig. 1). It must be noticed that from 2 patients with CML in accelerated phase in one case majority of cells in culture were matured granulocytes, that is characteristic for CML, while in another case culture material was presented by abundance of immature myeloid cells – myeloblasts, promyelocytes and myelocytes and a few band and segmented granulocytes that pointed to tumor progression. In the last case treatment was not effective at all.
Fig 1. Abundance of band neutrophils with ring nuclei. 2-day- bone marrow culture of a patient with CML started with blast crisis. Rapid maturation of blast cells up to band neutrophils in vitro enabled to diagnose CML. May-Grünwald –Giemsa stain. ? 1000.
Summary
Results of our study show that blood and bone marrow culture data of patients with CML can be successfully used as additional criteria for the differentiation of CML started with blast crisis from AML as far as in cultures of patients with AML abundant proliferation of blast cells is observed, whereas in the cases of CML started with blast crisis rapid maturation of blast cells up to band neutrophils from the beginning of cultivation is obvious. Abundance of immature cells in blood or bone marrow cultures of patients with CML points to tumor progression in spite of the clinical stage of disease and represents a bad prognostic marker. Cytochemical study or immunophenotyping of proliferated in vitro cells can help to determine the type of new proliferative clone.
Keyword(s): Acute myeloid leukemia, Chronic myeloid leukemia, Diagnosis, In vitro expression
Session topic: Publication Only
Abstract: PB1738
Type: Publication Only
Background
Despite the achievements of modern medicine sometimes there is a problem to differentiate chronic myeloid leukemia (CML) started with blast crisis from acute myeloblastic leukemia (AML), especially in the cases of Ph chromosome negative or BCR-ABL1- negative cases. Even in the presence of this marker one should have taken in mind that there are cases of Ph + AML as well.
Aims
The aim of our study was to precise the diagnose in patients with blast cells in peripheral blood and prominent hepato- and splenomegaly suspicious on CML and reveal additional criteria for the diagnosis of CML started with blast crisis.
Methods
To solve this problem we have used peripheral blood and bone marrow cell culture method worked out by us. This method supports propagation of blast cells specific for each form and variant of leukemia and enables to reveal the malignant clone according to morphocytochemical investigation or phenotyping in vitro proliferating cells (Shvelidze, Saralidze et al. Atlas of Hematology, 2013. http://www.e-bookland.ge/Books/medical/ATLAS-of-HEMATOLOGY). We investigated peripheral blood and bone marrow cell cultures of 5 patients with CML presented with blast crisis at the time of diagnosis, 8 patients with CML at chronic stage, 2 patients with CML in accelerated phase and 7 patients with AML (3 cases of AML without maturation and 4 cases of AML with maturation).
Results
Our studies showed that in all cases of AML proliferation of blast cells is confirmed by abundance of blast cells in cultures during 2 weeks of cultivation and appearance of maturation part of them up to promyelocytes and myelocytes and rarely to the band neutrophils in late cultures. On contrary, in the cases of CML presented with blast crisis as well as in the cases of CML at chronic stage, rapid maturation of blast cells up to band neutrophils is obvious from the beginning of cultivation. Just from the second day of cultivation in cultures of patients with CML disappearance of blast cells and abundance of band and segmented granulocytes, mainly neutrophilic, but eosinophilic and basophilic also are observed (Fig. 1). It must be noticed that from 2 patients with CML in accelerated phase in one case majority of cells in culture were matured granulocytes, that is characteristic for CML, while in another case culture material was presented by abundance of immature myeloid cells – myeloblasts, promyelocytes and myelocytes and a few band and segmented granulocytes that pointed to tumor progression. In the last case treatment was not effective at all.
Summary
Results of our study show that blood and bone marrow culture data of patients with CML can be successfully used as additional criteria for the differentiation of CML started with blast crisis from AML as far as in cultures of patients with AML abundant proliferation of blast cells is observed, whereas in the cases of CML started with blast crisis rapid maturation of blast cells up to band neutrophils from the beginning of cultivation is obvious. Abundance of immature cells in blood or bone marrow cultures of patients with CML points to tumor progression in spite of the clinical stage of disease and represents a bad prognostic marker. Cytochemical study or immunophenotyping of proliferated in vitro cells can help to determine the type of new proliferative clone.
Keyword(s): Acute myeloid leukemia, Chronic myeloid leukemia, Diagnosis, In vitro expression
Session topic: Publication Only
Type: Publication Only
Background
Despite the achievements of modern medicine sometimes there is a problem to differentiate chronic myeloid leukemia (CML) started with blast crisis from acute myeloblastic leukemia (AML), especially in the cases of Ph chromosome negative or BCR-ABL1- negative cases. Even in the presence of this marker one should have taken in mind that there are cases of Ph + AML as well.
Aims
The aim of our study was to precise the diagnose in patients with blast cells in peripheral blood and prominent hepato- and splenomegaly suspicious on CML and reveal additional criteria for the diagnosis of CML started with blast crisis.
Methods
To solve this problem we have used peripheral blood and bone marrow cell culture method worked out by us. This method supports propagation of blast cells specific for each form and variant of leukemia and enables to reveal the malignant clone according to morphocytochemical investigation or phenotyping in vitro proliferating cells (Shvelidze, Saralidze et al. Atlas of Hematology, 2013. http://www.e-bookland.ge/Books/medical/ATLAS-of-HEMATOLOGY). We investigated peripheral blood and bone marrow cell cultures of 5 patients with CML presented with blast crisis at the time of diagnosis, 8 patients with CML at chronic stage, 2 patients with CML in accelerated phase and 7 patients with AML (3 cases of AML without maturation and 4 cases of AML with maturation).
Results
Our studies showed that in all cases of AML proliferation of blast cells is confirmed by abundance of blast cells in cultures during 2 weeks of cultivation and appearance of maturation part of them up to promyelocytes and myelocytes and rarely to the band neutrophils in late cultures. On contrary, in the cases of CML presented with blast crisis as well as in the cases of CML at chronic stage, rapid maturation of blast cells up to band neutrophils is obvious from the beginning of cultivation. Just from the second day of cultivation in cultures of patients with CML disappearance of blast cells and abundance of band and segmented granulocytes, mainly neutrophilic, but eosinophilic and basophilic also are observed (Fig. 1). It must be noticed that from 2 patients with CML in accelerated phase in one case majority of cells in culture were matured granulocytes, that is characteristic for CML, while in another case culture material was presented by abundance of immature myeloid cells – myeloblasts, promyelocytes and myelocytes and a few band and segmented granulocytes that pointed to tumor progression. In the last case treatment was not effective at all.
Fig 1. Abundance of band neutrophils with ring nuclei. 2-day- bone marrow culture of a patient with CML started with blast crisis. Rapid maturation of blast cells up to band neutrophils in vitro enabled to diagnose CML. May-Grünwald –Giemsa stain. ? 1000.
Summary
Results of our study show that blood and bone marrow culture data of patients with CML can be successfully used as additional criteria for the differentiation of CML started with blast crisis from AML as far as in cultures of patients with AML abundant proliferation of blast cells is observed, whereas in the cases of CML started with blast crisis rapid maturation of blast cells up to band neutrophils from the beginning of cultivation is obvious. Abundance of immature cells in blood or bone marrow cultures of patients with CML points to tumor progression in spite of the clinical stage of disease and represents a bad prognostic marker. Cytochemical study or immunophenotyping of proliferated in vitro cells can help to determine the type of new proliferative clone.
Keyword(s): Acute myeloid leukemia, Chronic myeloid leukemia, Diagnosis, In vitro expression
Session topic: Publication Only
{{ help_message }}
{{filter}}