
Hematology

Contributions
Type: Publication Only
Background
A new MPN registry,based on the database of available patient data and a disease specific questionnaire were conducted and used in several Hungarian hematology centers.
Aims
The aim of the survey was to collect data of Philadelphia negative MPN patients, in order to establish a Hungarian MPN registry.
Methods
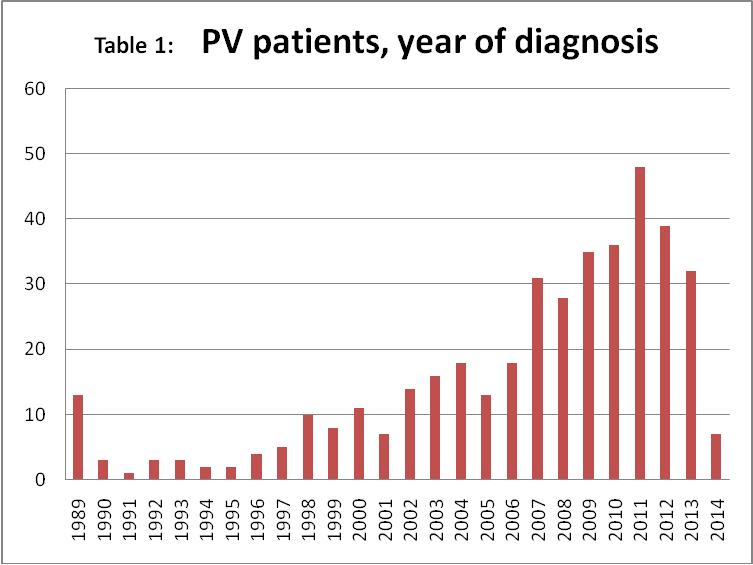
There was close cooperationbetween hematologists and information technicians (IT) experts to create an easily evaluable questionnaire. Data of classical MPN patients were collected from Hungarian centers. The thrombotic risk and the risk adapted treatment characteristics were stratified according to the Landolfi criteria. In this review the data of 408 patients (57% male) registered as having PV,were analysed. The data entry (Table 1)started at 2014 and the centers entered their patients data, diagnosed between 1989-2014.
Results
There were 820 evaluable MPN patients till the initial assesment deadline(15th Feb 2015) In the 408 evaluable PV pts the average time from diagnosis was 7.6 years, and about 50% of them were diagnosed more than 5 years ago. The number of evaluable cumulative patient years was 3016.
Among the 408 PV patients there were 80%(327) JAK2 V617F positive,13%(52) of them were JAK2 V617F negative. JAK status was missing in 7%(29)of patients.The detailed analysis of the JAK negative group revealed that 6 of them had an elevated hemoglobin + 2 positive minor criteria, fulfilling the 2008 WHO criteria, therefore they had proven PV.The other 67 patients did not fulfill the WHO diagnostic criteria of PV,they were identified as „insufficient” and therefore their data have not been included into the present evaluation.
According to the Landolfi thrombotic risk stratification there were 73 patients stratified as low/moderate risk. They have to be treated with phlebotomy and ASA only. 44 (60%) of them were treated with phlebotomy and only 25(34%) with ASA. 45(62%) of them were treated with cytoreductive drugs-mainly with hydroxyurea 36pts(49%), 1 with a JAK inhibitor,1 with anagrelide,and 1 with HU+anagrelide+ASA combination. Seven pts.(10%) received interferon-alfa. Among them 8 thrombotic events and no transformation was observed, thus, according to the
Landolfi risk treatment criteria, patients in this group were overtreated.
In the high /extremely high risk group there were 260 patients. 35% had thrombotic events prior to diagnosis. 32% had a thrombotic event after the diagnosis. Disease transformation has been found in 10% of the patients ( MF 22 pts, AML 2 pts, lymphoproliferative neoplasia in two patients.) 6% of registered PV patients had bleeding episodes
Summary
The main aim of the questionnaire was to create a national registry of MPN patients and to help our colleagues how to stratify the thrombotic risk and to choose the proper treatment. To date it remains unanswered whether low risk patients need cytoreductive treatment to prevent thrombotic events? Our data show an increase of thrombotic events in low risk patients treated with cytoreductive drugs (8 pts treated with cytoreductive drugs versus no patient treated with phlebotomy and ASA), thus arguing against treating these patients with cytoreductive drugs.Our results show the risk of thrombotic and hemorrhagic complications in PV to be comparable to published results. Based on our data we are convinced that the new national registry helps to give a good feedback about our diagnostic and treatment habits in PV.
Keyword(s): Aspirin, Hydroxyurea, Polycythemia vera, Thromboembolic events
Session topic: Publication Only
Type: Publication Only
Background
A new MPN registry,based on the database of available patient data and a disease specific questionnaire were conducted and used in several Hungarian hematology centers.
Aims
The aim of the survey was to collect data of Philadelphia negative MPN patients, in order to establish a Hungarian MPN registry.
Methods
There was close cooperationbetween hematologists and information technicians (IT) experts to create an easily evaluable questionnaire. Data of classical MPN patients were collected from Hungarian centers. The thrombotic risk and the risk adapted treatment characteristics were stratified according to the Landolfi criteria. In this review the data of 408 patients (57% male) registered as having PV,were analysed. The data entry (Table 1)started at 2014 and the centers entered their patients data, diagnosed between 1989-2014.
Results
There were 820 evaluable MPN patients till the initial assesment deadline(15th Feb 2015) In the 408 evaluable PV pts the average time from diagnosis was 7.6 years, and about 50% of them were diagnosed more than 5 years ago. The number of evaluable cumulative patient years was 3016.
Among the 408 PV patients there were 80%(327) JAK2 V617F positive,13%(52) of them were JAK2 V617F negative. JAK status was missing in 7%(29)of patients.The detailed analysis of the JAK negative group revealed that 6 of them had an elevated hemoglobin + 2 positive minor criteria, fulfilling the 2008 WHO criteria, therefore they had proven PV.The other 67 patients did not fulfill the WHO diagnostic criteria of PV,they were identified as „insufficient” and therefore their data have not been included into the present evaluation.
According to the Landolfi thrombotic risk stratification there were 73 patients stratified as low/moderate risk. They have to be treated with phlebotomy and ASA only. 44 (60%) of them were treated with phlebotomy and only 25(34%) with ASA. 45(62%) of them were treated with cytoreductive drugs-mainly with hydroxyurea 36pts(49%), 1 with a JAK inhibitor,1 with anagrelide,and 1 with HU+anagrelide+ASA combination. Seven pts.(10%) received interferon-alfa. Among them 8 thrombotic events and no transformation was observed, thus, according to the
Landolfi risk treatment criteria, patients in this group were overtreated.
In the high /extremely high risk group there were 260 patients. 35% had thrombotic events prior to diagnosis. 32% had a thrombotic event after the diagnosis. Disease transformation has been found in 10% of the patients ( MF 22 pts, AML 2 pts, lymphoproliferative neoplasia in two patients.) 6% of registered PV patients had bleeding episodes
Summary
The main aim of the questionnaire was to create a national registry of MPN patients and to help our colleagues how to stratify the thrombotic risk and to choose the proper treatment. To date it remains unanswered whether low risk patients need cytoreductive treatment to prevent thrombotic events? Our data show an increase of thrombotic events in low risk patients treated with cytoreductive drugs (8 pts treated with cytoreductive drugs versus no patient treated with phlebotomy and ASA), thus arguing against treating these patients with cytoreductive drugs.Our results show the risk of thrombotic and hemorrhagic complications in PV to be comparable to published results. Based on our data we are convinced that the new national registry helps to give a good feedback about our diagnostic and treatment habits in PV.
Keyword(s): Aspirin, Hydroxyurea, Polycythemia vera, Thromboembolic events
Session topic: Publication Only