
Hematology

Contributions
Type: Publication Only
Background
CMML is a clonal disease characterized by high rate progression to AML. Treatment is not curative traditionally and allo-SCT remains the only option, although in a minority of patients. Recently, significant clinical benefits by hypomethylating agents have been reported.
Aims
To evaluate efficacy and toxicity of azacitidine on CMML.
Methods
Fourteen patients with a median age of 75 (60-85) and several co-morbidities were evaluated; 5/14 (37%) aged > 80 years. Median PS was 70% (range 50-90). According to WHO, 10, 2 and 2 patients presented CMML-2, CMML-1 with severe and symptomatic cytopenias and CMML-related AML with <30% BM blasts, respectively. Six patients had proliferative CMML, 7 were transfusion-dependent at the start of azacitidine and two had abnormal karyotype. Three patients had CMML secondary to low risk MDS; one patient presented a therapy-related CMML. Previous therapies were: intensive chemotherapy (1), ESA (6) and hydroxyurea (8); 4 patients were treatment-naïve. The interval between diagnosis and the start of azacitidine was 2 months (0.3 – 18) and the median number of courses was 12 (2-33). Treatment was well-tolerated and with no remarkable side effects. Responses were evaluated according to 2006 IWG.
Results
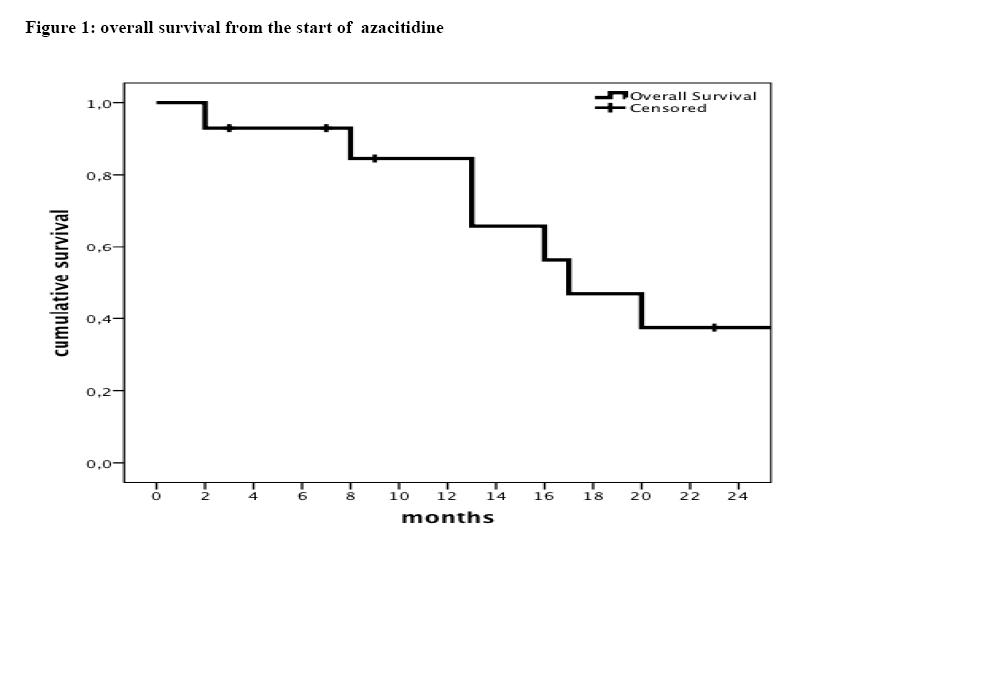
Thirteen patients were evaluable for response after the fourth cycle of azacitidine; the remaining patient developed AML after the second cycle of therapy. Five patients (36%) achieved CR and 6 (43%) PR with an ORR of 78%; two patients presented a primary failure to azacitidine. After a median follow-up of 19 months (5-46), 6 patients (3 in PR, 2 in CR and 1 with AML) are still alive, with an OS from CMML diagnosis and the start of azacitidine treatment of 25 and 17 months, respectively. Among responding patients, 1 is alive and well 120 days after unrelated allo-SCT. Six patients progressed to AML: 1 was primarily unresponsive to azacitidine and 5 progressed after 17 (5-40) months from the start of therapy. Among the 8 deceased patients, 5 died from AML progression and 3 because of complications related to pre-existing cardiac comorbidities (2 patients), or secondary lung cancer (1 patient).
Summary
Despite the limited number of cases, the results are encouraging, considering age and the complexity of the patients. The ORR of 78% and the unfavorable prognosis of our comorbid patients reinforce the existing evidence, making azacitidine the most appropriate treatment of CMML in the real life setting.
Keyword(s): Chronic myelomonocytic leukemia, Clinical outcome, Hypomethylation
Type: Publication Only
Background
CMML is a clonal disease characterized by high rate progression to AML. Treatment is not curative traditionally and allo-SCT remains the only option, although in a minority of patients. Recently, significant clinical benefits by hypomethylating agents have been reported.
Aims
To evaluate efficacy and toxicity of azacitidine on CMML.
Methods
Fourteen patients with a median age of 75 (60-85) and several co-morbidities were evaluated; 5/14 (37%) aged > 80 years. Median PS was 70% (range 50-90). According to WHO, 10, 2 and 2 patients presented CMML-2, CMML-1 with severe and symptomatic cytopenias and CMML-related AML with <30% BM blasts, respectively. Six patients had proliferative CMML, 7 were transfusion-dependent at the start of azacitidine and two had abnormal karyotype. Three patients had CMML secondary to low risk MDS; one patient presented a therapy-related CMML. Previous therapies were: intensive chemotherapy (1), ESA (6) and hydroxyurea (8); 4 patients were treatment-naïve. The interval between diagnosis and the start of azacitidine was 2 months (0.3 – 18) and the median number of courses was 12 (2-33). Treatment was well-tolerated and with no remarkable side effects. Responses were evaluated according to 2006 IWG.
Results
Thirteen patients were evaluable for response after the fourth cycle of azacitidine; the remaining patient developed AML after the second cycle of therapy. Five patients (36%) achieved CR and 6 (43%) PR with an ORR of 78%; two patients presented a primary failure to azacitidine. After a median follow-up of 19 months (5-46), 6 patients (3 in PR, 2 in CR and 1 with AML) are still alive, with an OS from CMML diagnosis and the start of azacitidine treatment of 25 and 17 months, respectively. Among responding patients, 1 is alive and well 120 days after unrelated allo-SCT. Six patients progressed to AML: 1 was primarily unresponsive to azacitidine and 5 progressed after 17 (5-40) months from the start of therapy. Among the 8 deceased patients, 5 died from AML progression and 3 because of complications related to pre-existing cardiac comorbidities (2 patients), or secondary lung cancer (1 patient).
Summary
Despite the limited number of cases, the results are encouraging, considering age and the complexity of the patients. The ORR of 78% and the unfavorable prognosis of our comorbid patients reinforce the existing evidence, making azacitidine the most appropriate treatment of CMML in the real life setting.
Keyword(s): Chronic myelomonocytic leukemia, Clinical outcome, Hypomethylation